Ancel Keys ~ It's Time to Appreciate a Real Researcher ...
... or at least stop lying about him and promoting bad research reviews.
Around a year ago, a "commissioned and internally peer reviewed" Editorial appeared in the British Medical Journal's off-shoot Open Heart online journal. The author, James J DiNicolantonio is identified as a Cardiovascular research scientist and PharmD, and he is also an Associate Editor of the journal.

This is a fledgling online journal conceived in 2013, and it is what I prefer to refer to as a "pay to play" publication. $3000 USD per article to be exact.

Here's a suggestion on a format change to demonstrate how dedicated you are to "maximum transparency": under Author Affiliations please list Associate Editor of This Journal!!! This particular Editorial/Review/Article (there really is no distinction where DiNicolantonio's ten or so contributions to Open Heart are concerned), is listed as "commissioned, internally reviewed". So he didn't have to pay to play, and may have been paid. Again, perhaps to "maximize" that transparency, this information should also be included right up front under Author Affiliations, so readers don't have to go looking for it at the end, if they even know it's there.
Ahh, but the whole Open Heart journal and "researchers" like DiNicolantonio will be a subject for a different day. Let's return to the article at hand. After praising Malhotra (sigh) as "refreshing", here is the second paragraph:
History of the low-fat ‘diet-heart’ hypothesis
The vilification of saturated fat by Keys [2] began two decades before the seven countries study, where Keys showed a curvilinear association between fat calories as a percentage of total calories and death from degenerative heart disease from six countries. However, he excluded data from 16 countries that did not fit his hypothesis. Indeed, data were available at the time from 22 countries, and when all countries were looked at the association was greatly diminished. [3] Furthermore, no association existed between dietary fat and mortality from all causes of death. Thus, past data promoted by Keys showing that an increased percentage of fat calories consumed increases the risk of death are not valid (and certainly could never have proved causation). These data seemingly lead us down the wrong “dietary-road” for decades to follow, as pointed out by others.
Stop.
Enough.
Whatever "vilification of saturated fat" Ancel Keys may have had a scientific hand in during the course of his career, it ABSOLUTELY DID NOT begin with Reference 2: Athersclerosis: A Problem in Newer Public Health ( ← link to full text, free!) I know it's long, but it's an interesting read, far more interesting that Good Calories, Bad Calories. Saturated fat is not even mentioned in that talk/paper. Not even mentioned. Did DiNicolantonio read it? I doubt it. The next two sentences smack of parroting the interpretations of others, and editorial or not, it seems in poor form to start out by impugning the character of a scientist of Keys' caliber. DiNicolantonio joins the ranks of countless others* in advancing the ignorant slander of Keys by one Gary Taubes. It has been implied that Keys willfully excluded data from 16 of 22 countries "that didn't fit his hypothesis".** Yerushalmy & Hilleboe never leveled such an accusation against Keys, though to be fair, they strongly implied it. At the very least the referencing needed to be more clear to indicate that this statement is DiNicolantonio's opinion (or that of whomever's views he co-opted), not some fact in the evidentiary record.
*This link is to an amazing compilation by Seth over at The Science of Nutrition blog. If you haven't read it yet, please do. It might just open your eyes a bit.
**In the past, I too, have been guilty of passing along the accusation of cherry-picking, mostly because I took on faith that the side-by-side images from Uffe Ravnskov, repeated incessantly around the IHC, were indeed valid. I was called out here once or twice, looked into it, looked some more, etc. If Seth's article isn't the last word on this nonsense, perhaps let this one be. ;-)
YERUSHALMY & HILLEBOE REVISITED
Let me preface this section by stating that it's been a while since I read some other's work on this topic, so some of this may have already been said, or perhaps I'm even repeating myself. To my recollection, however, many of the points I'm making here have not been made, at least in the same manner, before. If any of this is a repeat, I think it doesn't hurt to do so, but if I'm accidentally cribbing off of you without attribution, please let me know in comments so that I can correct myself and link up to your work!
Before moving on, I think it is important to revisit Yerushalmy & Hilleboe's data, and those 22 countries. In doing so again on my own accord, I have uncovered some errors and omissions that I feel are worthwhile discussing. Let's begin with the FACT that ...
Yerushalmy & Hilleboe Did Their Analysis Using Different Data Entirely:
This is not an insignificant point. Folks reading DiNicolantonio, or Teicholz, or Bailor, or Taubes, etc. are led to believe that Keys merely "cherry picked" 6 countries out of 22 to construct his infamously near-perfect plot. This willful misrepresentation of events has repeatedly cast aspersions on Keys' character. It would have been an egregious thing for Keys to have had access to the same data sets and simply selected only those points that fit his hypothesis, while discarding those that did not. There is no evidence of this. Even Y&H only say so much as the following:
Since no information is given by Keys on how or why the six countries were selected for Fig. 1, it is necessary to investigate the association between dietary fat and heart disease mortality in all countries for which information is available.But as has been pointed out before, Keys DID give an explanation:
So far it has been possible to get fully comparable dietary and vital statistics data from 6 countries.
Y&H ignore this statement. They do not challenge it. And they didn't demonstrate it to be a misrepresentation by producing more data from the time period Keys used. Their "proceedings" article was presented at a conference in April of 1957. Their heart disease mortality data was from the WHO Annual Epidemiological Reports, 1950-1953. Both on their plot, and on a table in their appendix, the mortality data was identified as coming from a three year period from 1951-1953. Their food consumption data used for fat intake statistics came from the Food and Agriculture Organization of the United Nations, 1951-1954. In other words:
Yerushalmy & Hilleboe's data did not yet exist at the time Keys gave his talk in January of 1953.
These references appear to be single reports that span to include 1953 for mortality and 1954 for the diet data. You can't construct a scatter plot without data for both axes. Therefore, the earliest the x-axis diet data would have been available would have been 1955, at least two years after Keys gave his talk. Given as Keys' "published graph" was apparently the sole impetus for Yerushalmy & Hilleboe's dissertation on correlations and statistics, perhaps a better question might be:
Why didn't Yerushalmy & Hilleboe use all of the data supposedly available to Ancel Keys from 1948-1949?
 Keys could not have used and cherry picked from their data, but they could have produced additional data if it were available to Keys.
Keys could not have used and cherry picked from their data, but they could have produced additional data if it were available to Keys.In addition to the years, Yerushalmy and Hilleboe used data from a different classification of heart disease. In the caption on Keys' famous graph, he notes that his data is for mortality rates for "Degenerative Heart Disease", and he specifies these are Categories 93 and 94 for 1938 data, and Categories 420 and 422 for 1948 data. Y&H used data from Category B-26. The screenshot at right contains all the pertinent information. For the Keys 6, they show the breakdown of B-26 into subcategories. That Keys' data didn't include endocarditis (421) would have made little difference in most cases, but this explains why Japan is higher on Y&H's plot than Keys'. Why didn't Yerushalmy & Hilleboe itemize out the data for the other 16 countries? Perhaps this, too, was not available to A.Ben?
We are left without an explanation, despite some rather painstaking detail and "what if" scenarios, as to why Yerushalmy and Hilleboe didn't just use Keys' data if it were available. Of course it would have made sense for them to use the most recent data they could get were the point of their article to present up-to-date information and to discuss/debate the diet-heart hypothesis. But there would have been no reason not to use slightly outdated data to discuss the finer points of statistical correlations ... it would have removed much ambiguity from their discussions. It seems rather the more unconscionable for them to have implied that their numbers were merely additional values, available to Keys. To repeat, this precedes their own Figure 3.
Since no information is given by Keys on how or why the six countries were selected for Fig. 1, it is necessary to investigate the association between dietary fat and heart disease mortality in all countries for which information is available.

This is shown in Figure 3 for males aged fifty-five to fifty-nine years in 22 countries.† It is immediately obvious that the inclusion of all the countries greatly reduces the apparent association.
 That clearly implies cherry picking. I have taken Keys' original plot for just this age group and through the magic of screen shots and Paint, rescaled and superimposed the 6 countries from the original plot in Y&H (enhanced data points with larger red dots). Clearly if you use different data, for the same 6 countries, the association is already significantly "reduced".
That clearly implies cherry picking. I have taken Keys' original plot for just this age group and through the magic of screen shots and Paint, rescaled and superimposed the 6 countries from the original plot in Y&H (enhanced data points with larger red dots). Clearly if you use different data, for the same 6 countries, the association is already significantly "reduced".In the end, while Yerushalmy and Hilleboe make no attempt to hide the source of their data, they made statements that would lead readers to believe they were merely supplementing Keys' data with additional information he neglected to include. This false impression was siezed upon most prominently by Gary Taubes, who twisted the facts further, and has been repeated by others ever since. But was Taubes the first?
Yerushalmy & Hilleboe's Data Has Morphed ...
The side by side image below, from Uffe Ravnskov's Cholesterol Myths, published in 2000, is ubiquitous on the internet. Here it is in a March 2011 post by Chris Masterjohn.
 |
Others had long since pointed out to me that the points from Figure 1A (Keys) do not overlay those from Figure 1B (Yerushalmy & Hilleboe). |
According to Dr. Keys, fat food was the culprit. His proof was a diagram, which showed that the intake of fat food and the death rates from coronary heart disease followed each other closely in six countries (fig. 1A). The points of the diagram lay as on a string, so that the curve he had drawn looked more like the result of a physical experiment than a biologic relationship. If you prolong the curve at the left it intersects the origin (= the intersection of the axes), thus suggesting that if you avoid fat food completely you will never have a coronary. Wrote a commentator in The Lancet the following year, ”The curve shows an almost convincing relationship between the fat content of the food and the risk of dying from coronary heart disease.”
But why did Dr. Keys use the figures from six countries only? At that time information was available from 22 countries and if all of them were included the association was in fact rather weak. For instance, the death rate from coronary heart disease in some countries was 3-4 times higher than in countries where the consumption of fat was the same (fig. 1B).
~ Uffe Ravnskov, MD, PhD The Cholesterol Myths
Where did Ravnskov get this idea? Yerushalmy and Hilleboe perhaps? Given the incestral nature of the players in the ancestral community, it seems entirely plausible that this "cherry picking" charge originated with Ravnskov and Taubes merely put his "flare" on it in GCBC:
Many researchers wouldn’t buy it. Jacob Yerushalmy, who ran the biostatistics department at the University of California, Berkeley, and Herman Hilleboe, the New York State commissioner of health, co-authored a critique of Keys’s hypothesis, noting that Keys had chosen only six countries for his comparison though data were available for twenty-two countries. When all twenty-two were included in the analysis, the apparent link between fat and heart disease vanished.
The reason I bring Rasnkov into this is because his plots are of higher quality than the original Y&H plot so I began with playing around with them as a substitute for the original. I was also trying to reconcile some issues with Y&H's data -- I'll get to that in a bit here -- and decided I needed to work with the original. The figures below are from what appears to be a newer ebook version. Ravnskov has updated his plots. I've screen shot this and cobbled it together a bit for display here, but it is interesting that his overlay no longer exists.

However, here are some more interesting overlays. The Ravnskov data from the current Fig 1B(blue dots) doesn't match up very well at all with that of yesteryear (left), nor does it appear to jive with Y&H's data (middle). Although it's the best match of all, Ravnskov's original plot didn't match completely with Y&H's either (right). Tsk tsk.

Ancel Keys Stunk At Cherry Picking!
Alrighty then! Here's another question. Let's assume that Keys really did have access to a pool of data from 22 countries. Why would he have picked those six countries? It is often repeated, and is now published in Open Heart journal of the BMJ journal family, that Keys selected only those countries that supported his hypothesis, and he left off those that did not. But this does not even make sense! Certainly there were others, and more of them, that would have created a better fit, and an even more pronounced effect! Below right, I selected data from 14 countries (Australia, Austria, Canada, Ceylon, Chile, Germany, Ireland, Italy, Japan, New Zealand, Portugal, Switzerland, UK and US) that would have been even more convincing than what Keys presented!

IF Keys had tried to use Y&H's data to his advantage, it would have been unlikely he would have chosen the same six points. This accusation is not only inappropriate and beneath serious scientists, it's also pretty absurd on its face if you look at the data.
IF Keys had tried to use Y&H's data to his advantage, it would have been unlikely he would have chosen the same six points. This accusation is not only inappropriate and beneath serious scientists, it's also pretty absurd on its face if you look at the data.
Errors and Missing Numbers in Yerushalmy & Hilleboe
 I was trying to quickly estimate the values off of Y&H's plot to do a +/- type analysis about the 30% fat line. Then I remembered that Y&H include data in their Appendix. I didn't pay much attention to the disease class and just constructed a quick table and plot in Excel using their data. Lo and behold, it did not overlay their plot very nicely. So I looked more closely and discovered that the data in the Appendix for mortality was for B26+B27 combined. The plot is clearly for only B26. Now I realize that Ravnskov did the same thing His points perfectly overlay mine, no wonder he didn't do the overlay on Keys' data! (Though I wonder what he was thinking when he updated his plot!)
I was trying to quickly estimate the values off of Y&H's plot to do a +/- type analysis about the 30% fat line. Then I remembered that Y&H include data in their Appendix. I didn't pay much attention to the disease class and just constructed a quick table and plot in Excel using their data. Lo and behold, it did not overlay their plot very nicely. So I looked more closely and discovered that the data in the Appendix for mortality was for B26+B27 combined. The plot is clearly for only B26. Now I realize that Ravnskov did the same thing His points perfectly overlay mine, no wonder he didn't do the overlay on Keys' data! (Though I wonder what he was thinking when he updated his plot!)  I was about to resort to guesstimating values when I noticed this table in the text. Perhaps it's just irony that in a paper/talk dedicated in many ways to minutia (not all, but some), Y&H committed a faux pas or few of their own. Note that B-26 is arteriosclerotic and other degenerative heart disease and B-27 is all other heart disease. The data reported in the Appendix is for B-26 and B-27 combined. Table II here has the categories itemized for only 13 of the 22 countries. The plot is clearly for B-26 only, so that all of the data exists somewhere. I find it odd that for this major plot to compare to Keys', Yerushalmy and Hilleboe opted not to provide the full data for all 22 countries. They bothered to itemize it for some countries. Things that make you go hmmm? In addition, they had some data to itemize the 420/421/422 classification data for the B-26 classification. Did they have this for all countries? If they did, why didn't they make a plot of that data (420 and 422, as indicated was Keys' plot). Point being, that despite harping on how it can influence the data to in/exclude different classes, and for all their seeming rigor, Y&H's data selection and presentation doesn't seem to meet their own standards.
I was about to resort to guesstimating values when I noticed this table in the text. Perhaps it's just irony that in a paper/talk dedicated in many ways to minutia (not all, but some), Y&H committed a faux pas or few of their own. Note that B-26 is arteriosclerotic and other degenerative heart disease and B-27 is all other heart disease. The data reported in the Appendix is for B-26 and B-27 combined. Table II here has the categories itemized for only 13 of the 22 countries. The plot is clearly for B-26 only, so that all of the data exists somewhere. I find it odd that for this major plot to compare to Keys', Yerushalmy and Hilleboe opted not to provide the full data for all 22 countries. They bothered to itemize it for some countries. Things that make you go hmmm? In addition, they had some data to itemize the 420/421/422 classification data for the B-26 classification. Did they have this for all countries? If they did, why didn't they make a plot of that data (420 and 422, as indicated was Keys' plot). Point being, that despite harping on how it can influence the data to in/exclude different classes, and for all their seeming rigor, Y&H's data selection and presentation doesn't seem to meet their own standards.
But wait! There's more. I put the data provided for categoties B-26 and B-27 separately from Table II, along with the combined data from the Appendix into a spreadsheet to create a plot. Curious to make sure it coincided, I added the values to compare, and discovered that for 1 of the 13 countries, it didn't add up. I suppose one could forgive this, but it is a pretty substantial inconsistency, and not only that, it is for one of the Keys-6 countries, namely Italy: B-26 = 428, B-27 = 40 (adds to 468) ; Reported B26+B27 = 283. Odd, no?

It's only one of 13 data points, but it was Italy, and what assurances do we have that similar errors aren't lurking in the other 9 countries? Might seem nit picky but the 428 wasn't likely an issue of transposed digits of 248. All of the other combined values were within ±1. Is this an error in the WHO data or Y&H's version? To me this casts more doubt on the rigor of Y&H's analyses as we don't have ALL of the hard data they used to know.
It's only one of 13 data points, but it was Italy, and what assurances do we have that similar errors aren't lurking in the other 9 countries? Might seem nit picky but the 428 wasn't likely an issue of transposed digits of 248. All of the other combined values were within ±1. Is this an error in the WHO data or Y&H's version? To me this casts more doubt on the rigor of Y&H's analyses as we don't have ALL of the hard data they used to know.
Summary of Keys vs. Yerushalmy & Hilleboe:
- Y&H's data did not exist at the time Keys did his analysis
- Y&H chose to use different data instead of "all of the countries" for which data were supposedly available to Keys
- Y&H's data for the 6 Countries already differ from Keys' data
- Data included in Y&H's paper is incomplete and contains at least one inconsistency.
Continuing with the editorial:
Keep in mind that Keys himself only concluded as follows:
Whether or not cholesterol level, etc., are involved, it must be concluded that dietary fat somehow is associated with cardiac disease mortality, at least in middle age.So continuing on with DiNicolantonio's introduction ...
The vilification of saturated fat by Keys began two decades before the seven countries study, where Keys showed a curvilinear association between fat calories as a percentage of total calories and death from degenerative heart disease from six countries. However, he excluded data from 16 countries that did not fit his hypothesis. Indeed, data were available at the time from 22 countries, and when all countries were looked at the association was greatly diminished. Furthermore, no association existed between dietary fat and mortality from all causes of death.[3] Thus, past data promoted by Keys showing that an increased percentage of fat calories consumed increases the risk of death are not valid (and certainly could never have proved causation). These data seemingly lead us down the wrong “dietary-road” for decades to follow, as pointed out by others.
What is the point of including the statement about all cause mortality? I could let it go, but one of the major points made by Yerushalmy and Hilleboe was that if we look at all the various categories and such, there are greater associations to be made between other dietary components and heart disease mortality. No association with all cause? True, but a greater association for animal protein and animal fat than for total fat, and a negative association for vegetable fat and carbohydrate to boot! Not to mention the strongest correlation of all being for total calories.
DiNicolantonio's editorial was in a cardiovascular journal after all. It was about cardiometabolic consequences of dietary composition, says so right there in the title. Yerushalmy and Hilleboe's point is a debatable one at best. One can look at epidemiological data for which we have more accurate measures than for diet (e.g. LDL, LDL-P, apoB, HbA1c ...) and find predictive associations for all manner of diseases that do not translate to all cause mortality. So what's the point? There isn't one, except to distract. In the end:
- Yerushalmy and Hilleboe found a statistically significant association between Total Dietary Fat (in Calorie %) and death from Degenerative Heart Disease (B-26) in the 22 Countries for which they had data.
- Keys never reported a correlation coefficient, but his association was visibly greater than Y&H found for more, and different, data.
Let's repeat DiNicolantonio's next statement from that paragraph:
Thus, past data promoted by Keys showing that an increased percentage of fat calories consumed increases the risk of death are not valid (and certainly could never have proved causation).
Keys said nothing about risk of death in general. His focus was death by heart attack from degenerative heart disease. This is not a nit pick. Keys himself was very cautious in his wording in 1953. If DiNicolantonio is referring to later statements by Keys, he really needs to link to them directly. As it stands, he is referring to Keys-1953, and to repeat what Ancel Keys, himself, actually said:
W1hether or not cholesterol level, etc., are involved, it must be concluded that dietary fat somehow is associated with cardiac disease mortality, at least in middle age.
Since I repeated that, I note once again, that what is missing is equally important. That being the word "saturated". Keys did not "begin his vilification" of saturated fats in 1953. He didn't claim cause.
The Wrong Dietary Road ...
So as the story goes, by hook or by crook Ancel Keys convinced the world to reduce their fat intake to 30%, which all dutifully obeyed, and the consequences have been myriad. Putting it all back together, and focusing on DiNicolantonio's last sentence:
The vilification of saturated fat by Keys began two decades before the seven countries study, where Keys showed a curvilinear association between fat calories as a percentage of total calories and death from degenerative heart disease from six countries. However, he excluded data from 16 countries that did not fit his hypothesis. Indeed, data were available at the time from 22 countries, and when all countries were looked at the association was greatly diminished. Furthermore, no association existed between dietary fat and mortality from all causes of death. Thus, past data promoted by Keys showing that an increased percentage of fat calories consumed increases the risk of death are not valid (and certainly could never have proved causation). These data seemingly lead us down the wrong “dietary-road” for decades to follow, as pointed out by others.4 ,5
Alrighty then, in reverse order, Reference 5 is from none other than Principal Involuntary Content Contributor at The Carb-Sane Asylum: Mr. Gary Taubes. Perhaps to avoid anyone noticing the Keys/Y&H similarities, a 2001 Science article entitled The Soft Science of Dietary Fat, instead of GCBC.
I can no longer take seriously ANYONE who declares a modest suggestion -- reducing total fat to 30% of calories -- is in any way extreme or dangerous. In the early 1950's, 10 of these 22 countries met that mark. Always remember, this was no random or representative sampling of the global human diet. Countless accounts in the peer-review literature indicate the under-20% fat is woefully under-represented. Even France came in at 29%. So enough of that utter nonsense, OK? A couple of quick calculations:
 If we substitute the 250 from the plot for Italy, the low fat group mortality rates go to 228 and 251 for ≤ 30% and below median respectively.
If we substitute the 250 from the plot for Italy, the low fat group mortality rates go to 228 and 251 for ≤ 30% and below median respectively.
Show me the verifiable data for high rates of heart disease amongst all these low fat consuming countries.
Heck, let's go one step further, even if you average up to 33% fat group the mortality is 281 for average fat intake of 24.9%, while 35% on up group averaged mortality at 398 with 38.1% fat. Here's the other OBVIOUS thing about these 22 Countries -- 40% was the upper end of fat intake. NOT the average or norm.
Which brings us to the second citation regarding going down the wrong road. Which again ... would be the road that roughly half of a high-fat-loaded sampling of countries was already on?
So the final reference is a book: The Rise and Fall of Modern Medicine by James Le Fanu, M.D., "a medical columnist for the Daily Telegraph and Sunday Telegraph as well as a writer for the Times, the Spectator, and GQ. This book must be Robb Wolf's Bible. I haven't had time to read it all, but my Cliff's Notes take away is that modern medicine was the bomb when it eradicated infectious diseases and the like, but it's made barely any progress since. Really? I realize there are issues with what has happened with medicine, systems in different countries. I recognize that everyone wants to live a disease free life for, apparently, ever and modern medicine has failed miserably at that. But I'm really kind of sick and tired of those who think anyone taking any prescription med (other than metformin, which should probably be put in the water supply) that might be extending their life doesn't have "any sort of life worth living". That's horse manure and you know it!
Before discussing LeFanu's take on Keys I'd like to point out two things that jumped out at me from my brief skim:
Fear of fat
Leaving aside Taubes' confusing intermingling of almost 3 decades in time, look back at the 22 countries folks like Taubes and DiNicolantonio seem bound and determined to fixate upon. Let's look at the data just from that infamous plot. Do you notice anything? I made a pretty table for you to assist.During the first half of the 20th century, nutritionists were more concerned about malnutrition than about the sins of dietary excess. After World War II, however, a coronary heart disease epidemic seemed to sweep the country (see sidebar on p. 2540). “Middle-aged men, seemingly healthy, were dropping dead,” wrote biochemist Ancel Keys of the University of Minnesota, Twin Cities, who was among the first to suggest that dietary fats might be the cause. By 1952, Keys was arguing that Americans should reduce their fat intake to less than 30% of total calories, although he simultaneously recognized that “direct evidence on the effect of the diet on human arteriosclerosis is very little and likely to remain so for some time.” In the famous and very controversial Seven Countries Study, for instance, Keys and his colleagues reported that the amount of fat consumed seemed to be the salient difference between populations such as those in Japan and Crete that had little heart disease and those, as in Finland, that were plagued by it. In 1961, the Framingham Heart Study linked cholesterol levels to heart disease, Keys made the cover of Time magazine, and the AHA, under his influence, began advocating low-fat diets as a palliative for men with high cholesterol levels. Keys had also become one of the first Americans to consciously adopt a heart-healthy diet: He and his wife, Time reported, “do not eat ‘carving meat'—steaks, chops, roasts—more than three times a week.”
 |
| Gray values estimated from Figure 3 Black values from Table II, all shaded rows from Table II Italy may be in error, estimated B26 from Fig 3 is 250 |
I can no longer take seriously ANYONE who declares a modest suggestion -- reducing total fat to 30% of calories -- is in any way extreme or dangerous. In the early 1950's, 10 of these 22 countries met that mark. Always remember, this was no random or representative sampling of the global human diet. Countless accounts in the peer-review literature indicate the under-20% fat is woefully under-represented. Even France came in at 29%. So enough of that utter nonsense, OK? A couple of quick calculations:
≤ 30% (n=10): Avg. Fat Intake = 21.8% , Avg B-26 Mortality = 247
> 30% (n=12): Avg. Fat Intake = 36.2% , Avg B-26 Mortality = 400
< 31% Median: Avg. Fat Intake = 23.5% , Avg B-26 Mortality = 267
> 31% Median: Avg. Fat Intake = 37.2% , Avg B-26 Mortality = 407
If we substitute the 250 from the plot for Italy, the low fat group mortality rates go to 228 and 251 for ≤ 30% and below median respectively. Show me the verifiable data for high rates of heart disease amongst all these low fat consuming countries.
Heck, let's go one step further, even if you average up to 33% fat group the mortality is 281 for average fat intake of 24.9%, while 35% on up group averaged mortality at 398 with 38.1% fat. Here's the other OBVIOUS thing about these 22 Countries -- 40% was the upper end of fat intake. NOT the average or norm.
Which brings us to the second citation regarding going down the wrong road. Which again ... would be the road that roughly half of a high-fat-loaded sampling of countries was already on?
So the final reference is a book: The Rise and Fall of Modern Medicine by James Le Fanu, M.D., "a medical columnist for the Daily Telegraph and Sunday Telegraph as well as a writer for the Times, the Spectator, and GQ. This book must be Robb Wolf's Bible. I haven't had time to read it all, but my Cliff's Notes take away is that modern medicine was the bomb when it eradicated infectious diseases and the like, but it's made barely any progress since. Really? I realize there are issues with what has happened with medicine, systems in different countries. I recognize that everyone wants to live a disease free life for, apparently, ever and modern medicine has failed miserably at that. But I'm really kind of sick and tired of those who think anyone taking any prescription med (other than metformin, which should probably be put in the water supply) that might be extending their life doesn't have "any sort of life worth living". That's horse manure and you know it!
Before discussing LeFanu's take on Keys I'd like to point out two things that jumped out at me from my brief skim:
- LeFanu is not a big fan of diet causing diseases, nor conversely, apparently of altering diet as a means of preventing or curing them. He discusses this with regards to cancer, but also slips in a reference to Keys and the Japanese basically saying that if one switches their diet they may only be "switching the risk of dying from the types of cancer common in the West [and heart disease] to those common in Japan".
- The soaring popularity of Alternative Medicine is listed as one of four tell-tale paradoxes. LeFanu writes "The demonstrable success and effectiveness of modern medicine should have marginalised alternatives such as homeopathy and naturopathy into oblivion. Not so. In the United States there are more visits to providers of ‘unconventional therapy’ (425 million) than to ‘primary care physicians’ (388 million annually). As the efficacy of alternative therapies is not routinely tested in clinical trials (which does not mean they do not work), it is only natural to ask why the public should appear to have so much faith in them. {6}" Interestingly, this was written 15 years ago and referenced a 1993 NEJM article (see link). I just find it odd that DiNicolantonio hasn't left the pharmaceutical field in disgust by now ;-)
Returning to the subject of Ancel Keys and the "wrong dietary road", LeFanu writes:
Among those interested in solving the problem was Ancel Keys, the forty-year-old Director of the Laboratory of Physiological Hygiene at the University of Minnesota, who, at the close of the war, turned his attention to investigating why so many middle-aged men were dying from heart attacks. His particular scientific interest was nutrition, and so naturally enough he focused his attention on the chemical cholesterol present in the atheroma of the arteries. The main source of cholesterol is the liver, from where it is released into the bloodstream to fulfil its indispensable role as an integral part of the walls lining the cells, as well as being the precursor of many important hormones, including testosterone in the male and oestrogen in the female. Perhaps, Keys speculated, the other source of cholesterol – in food such as eggs and avocados – might, in combination with other fats, force up its level in the blood , which would then infiltrate the artery walls to form the atheroma that appeared to be implicated in heart attacks. It was not an original idea, but Ancel Keys was to pursue it so vigorously over the next years as essentially to make it his own. 9
Firstly, Le Fanu is an MD and that he doesn't know that avocados are essentially cholesterol free, is quite disturbing. Secondly, I hope everyone realizes by now, that even in his infamous 1953 paper, Keys was NOT speculating that the main cause of elevated blood cholesterol was dietary cholesterol. Reference 9 is to a 1941 publication entitled "Chinese Lessons in Medicine". But kudos are due to Le Fanu, as he is the first I've seen to mention Keys' first seminal work in this area of research: The Minnesota Businessman Study (my post on this forgotten "Other Minnesota Study") by citing the 23 year followup (Mortality and Coronary Heart Disease Among Men Studied for Twenty-three Years, Arch.Int.Med. 1971. 128:201-14 ... sadly cannot even find a link other than as a citation). Regardless, as refreshing as it is to see this study even mentioned, we are treated to yet another inventive timeline of events!
Perhaps if any of you reading this is familiar with this book you can confirm or deny for me whether my impression that this guy is a bit of a consipiracy type. After a disjointed, but more fair than most discussion of the trials of Keys and his ideas, the discussion turns to cholesterol lowering drugs. This is a separate issue, but it is a hot topic that hits nerves and riles people up.
However even if Americans had reduced fat intake (in total, not as a percent by upping carbs), the change is still to around 33%. Hardly some obscure lightly traveled path as dietary behavior goes. Eating more than 40%, now that would be a strange experiment indeed.
DiNicolantonio's editorial continues on in familar fashion -- saturated fats were replaced with refined carbs and crappy O6 oils, which is exactly what the dietary recommendations were, right? And look at these nominally better improvements in cardiometabolic parameters in weight loss trials, but LDL too high? We'll just become a skeptic for that, adopt another pet biomarker, make up and perpetuate still another (fluffy LDL anyone?!), and encourage folks down a totally untested dietary path.
Meanwhile they'll identify a different culprit, ignore any evidence that they are going down the wrong path, and encourage people to eat a diet that is foreign to the vast majority (one might say statistically 100%) of humans worldwide. And if/when it has deleterious long term consequences, then what will they do? Prescribe metformin?
DiNicolantonio has never done any primary research. He is not a scientific researcher. He joins a long line of similar who feel emboldened to take pot shots at real researchers like Ancel Keys. What is most ironic is that these folks, seemingly to a one, have preconceived ideas of their own. Ideas they continue to advance despite being presented with existing and convincing evidence to the contrary. In DiNicolantonio's case, there is a lot more to say on that point. Much has been said about the others, but if the past is any indication, there will continue to be a steady stream of material coming my way from them as well.
Perhaps if any of you reading this is familiar with this book you can confirm or deny for me whether my impression that this guy is a bit of a consipiracy type. After a disjointed, but more fair than most discussion of the trials of Keys and his ideas, the discussion turns to cholesterol lowering drugs. This is a separate issue, but it is a hot topic that hits nerves and riles people up.
However even if Americans had reduced fat intake (in total, not as a percent by upping carbs), the change is still to around 33%. Hardly some obscure lightly traveled path as dietary behavior goes. Eating more than 40%, now that would be a strange experiment indeed.
DiNicolantonio's editorial continues on in familar fashion -- saturated fats were replaced with refined carbs and crappy O6 oils, which is exactly what the dietary recommendations were, right? And look at these nominally better improvements in cardiometabolic parameters in weight loss trials, but LDL too high? We'll just become a skeptic for that, adopt another pet biomarker, make up and perpetuate still another (fluffy LDL anyone?!), and encourage folks down a totally untested dietary path.
Meanwhile they'll identify a different culprit, ignore any evidence that they are going down the wrong path, and encourage people to eat a diet that is foreign to the vast majority (one might say statistically 100%) of humans worldwide. And if/when it has deleterious long term consequences, then what will they do? Prescribe metformin?
Bottom Line:
DiNicolantonio has never done any primary research. He is not a scientific researcher. He joins a long line of similar who feel emboldened to take pot shots at real researchers like Ancel Keys. What is most ironic is that these folks, seemingly to a one, have preconceived ideas of their own. Ideas they continue to advance despite being presented with existing and convincing evidence to the contrary. In DiNicolantonio's case, there is a lot more to say on that point. Much has been said about the others, but if the past is any indication, there will continue to be a steady stream of material coming my way from them as well.
Comments
Is there a line of argument that the decreasing fat content (relative, not absolute) in the US diet had something to do with this?
http://www.marksdailyapple.com/saturated-fat-healthy/#axzz3RpZP8ae6
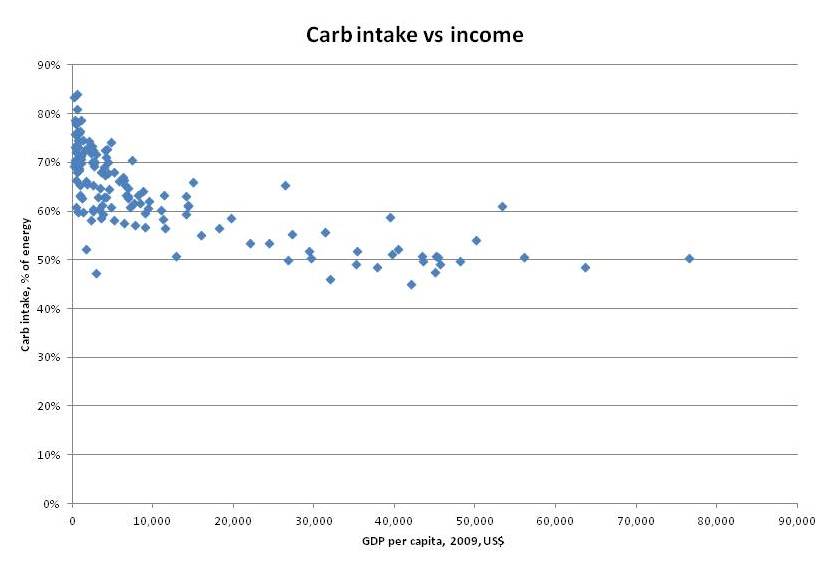
Peter@Hyperlipid as well
http://high-fat-nutrition.blogspot.com/2009/02/cholesterol-presentation-between.html
Cholesterol presentation: Between countries
http://high-fat-nutrition.blogspot.com/2007/11/professor-john-yudkin-and-dr-ancel-keys.html
Professor John Yudkin and Dr Ancel Keys
I think the lower
Also, according to Evelyn, Y&H included non atherosclerotic disease. Acquired valvular heart disease is both greatly reduced due to antibiotics and treated more effectively. Atherosclerotic valvular disease (aortic stenosis) is treated more effectively.
I took Charles' list as simply an FYI, here are some other sources. With the exception of Minger, it is doubtful there is much if any overlap there ;-)
The analogy is more apt than some may think. In 2008 Dr. Eric Westman encouraged one struggling low carber to:
1. Watch portion sizes (e.g. eat less overall) and
2. Eat more fat on a proportional basis
A certain someone translated this into eating more fat with a high protein meal and ignoring the advice on portion sizes.
With these multiple factors in play, opportunists feel they can take liberties to downplay or even absolve the guilt of saturated animal fat in the role of atherosclerosis? Perhaps they feel the other factors will cover for a shift back to massive saturated fat consumption???
Articles like DiNicolantonio's and books like BFS should also be seen in the context of total meat consumption taking a nosedive with the Great Recession and positive publicity about plant-based diets in general, and the Beef Checkoff Program developed in response. .
Adding fuel to the fire is the BMJ's predilection for controversy.
Www.specialtyhealth.com
The one that claims it saves $$ ???
Editorial: The Risk of Coronary Heart Disease
ANCEL KEYS
Circulation. 1961;23:805-812
Trends in
Dietary Intakes and Serum Cholesterol Levels over 50 Years in Tanushimaru in
Japanese Men
When I first got in trouble with the despicable Robb Wolf man-child it was related to this: http://www.donotlink.com/dqio (you'll note in the comments that he goes after Charles for inquiring about the program as well).
I asked a simple question on Twitter a week or so before his outburst as regards what exactly the diet was that Specialty Health was using. His answer was that he didn't know really, got the "you can call them" (why should I have to? You're promoting it as paleo, can't you give a hint?) before he finally gave a vague indication that it was a Lindeberg-esque (low fat, low sat fat) version of paleo.
Specialty Health uses diet (not Bulletproof) and STATINS and other medications (metformin, etc.) to normalize lipids. Their focus in on LDL particle number when LDL-C is often normal and trigs are also high. I am pretty sure that if LDL-C is high, they are on that like Jimmy on butter.
"As Dayspring said about the potato, if you're insulin resistant then you're not doing yourself any favours [eating fruit]. Doesn't matter how many micronutrients, phytochemicals, antioxidants they have in them, they are going to stimulate insulin secretion, they're going to cause your triglycerides to go up, fat to be accumulated ..."
How does Taubes think people get to be insulin resistant in the first place? He should look up 'magnesium deficiency insulin resistance'. Or 'copper deficiency insulin resistance'. Or 'iron overload insulin resistance', or 'manganese diabetes'. These things are not really in doubt any more.
Lipid Changes on a Very-Low-Carb Ketogenic Diet: My Own Experience
Authors:
Franziska Spritzler, RD, CDE
Thomas Dayspring, MD, FACP, FNLA
Published: August 2014
My NMR results indicate I have the large, pattern A type of LDL with a low number of the more atherogenic small LDL particles (small LDL-P).
All lipoprotein particles have finite diameters or sizes. All groups of specific lipoproteins are heterogeneous collections of variably sized particles. Since all lipoproteins undergo constant catabolism (liopolysis) the sizes are constantly changing from large to smaller species in everyone. LDLs vary in size from ~18 nanometers (nm) to 23 nm. Labs can report the peak particle size meaning the size of the predominant LDL species present. In reality most people have LDLs of all different sizes. An older term is LDL pattern or phenotype A or B, where the former means predominantly larger particles and the latter smaller particles. But most folks who are classified as Phenotype A will have some small LDLs and vice versa for those with Pattern B. Although one can find lots of literature as to why once they are in the artery wall, the small LDL may be particularly bothersome, including its susceptibility for oxidation; the standard graveyard has many persons who died of myocardial infarctions due to large LDLs. What drives an LDL into the arterial wall is primarily particle number not particle size. Any apoB particle with a diameter of < 70 nm can enter the arterial wall. The largest LDL is 23 nm, so when present in excess amounts any apoB particle will find its way into the arterial wall. People with FH who have, for the most part neither LDL particle size nor LDL cholesterol content is an independent risk factor for CHD risk once adjusted for LDL-P. So of course small LDLs are bad, when they exist in increased numbers --- but the same is true for large LDLs. One of the major reasons for increased LDL-P is the inability of the hepatic LDLr to clear the LDL particles
from plasma. Increasing the residence time of LDL will cause increased LDL-P. LDLr attach to LDLs at a specific area (domain) of the apoB on the surface of LDLs. As the size of an LDL becomes too small or too large, the domains on apoB become distorted and are not as readily recognized by LDLr leading to increased LDL-P. So to promote clearance the LDL size should be mid-range – neither too small nor too large. LDLs can be separated into over 15 sizes and only those of midsize are readily cleared. The most useful way to use LDL size is to recognize that the presence of increased small LDL is a good marker of them presence of insulin resistance.
https://twitter.com/HELPdietSA/status/568437593097908224/photo/1
http://www.businessinsider.com/our-war-on-fat-was-a-huge-mistake-graphs-2013-11
ScienceMore: Authority Nutrition Trans Fats Diet Weight Loss
6 Charts That Show How The War On Fat Was A Gigantic Mistake
KRIS GUNNARS, AUTHORITY NUTRITION
"If stress itself were really a leading cause of heart attacks, surely the number of heart attacks would have risen dramatically in Europe during World War II. But in fact the death rate from heart disease fell, as people from war-ravaged countries were forced by circumstance to eat less rich, high-fat, cholesterol-laden foods. In other words, it's demonstrably better for your heart to eat a low-fat, vegetarian diet while bombs drop all around you than to enjoy your steak in peace."
I've also seen a contention (with numbers) that the jump in heart disease in the US between about 1920 and 1960 coincided with a marked reduction in unrefined-carbohydrate consumption and a marked increase in animal-food consumption (with sugar intake being pretty much constant).
I do wonder about how stressful WWII was. My father was a fighter pilot and fought in the Battle of Britain. He was even shot down, but he only had good things to say about the war. He loved it. He never really adjusted to life afterwards, and took to fighting his family instead of Germans. It is my belief that this was more stressful than the war.
I think the stress connection is likely one of those that acts to exacerbate other causes. For example, if you're hypertensive, being stressed will make matters worse.
FWIW, during the war my Mom tells of how they would trade rations with American soldiers for other things they needed.
http://plantpositive.com/dietary-trends-1-nusi-guys-7/
http://www.nhlbi.nih.gov/about/documents/factbook/2011/chapter4#4_2
Obviously, for some groups of people the war was a nightmare. It can't have been much fun for my mother, in London with two small children and bombs falling, unable to contribute to the war effort and not knowing from day to day whether she'd see my father again.
Human Atherosclerosis and the Diet
By ANCEL KEYS, PH.D.
In summary, then, we may remark that direct evidence on the effect of the diet on human atherosclerosis is very little and is likely to remain unsatisfactory for a long time. But such evidence as there is, plus valid inferences from indirect evidence, suggests that a substantial measure of control of the development of atherosclerosis in man may be achieved by control of the intake of calories and of all kinds of fats, with no special attention to the cholesterol intake. This means: (1) avoidance of obesity, with restriction of the body weight to about that considered standard for height at age 25; (2) avoidance of periodic gorging and even temporary large calorie excesses; (3) restriction of all fats to the point where the total extractable fats in the diet are not over about 25 to 30 per cent of the total calories;
(4) disregard of cholesterol intake except, possibly, for a restriction to an intake less than 1 Gm. per week.
While such a trial could probably not be done today, we also don't even commit as many schizophrenics as we once did, and I'm not aware that those treated on an outpatient basis are unable to give informed consent to participate in a trial like anyone else.
Although Teicholz tried to portray this in an evil light in her book, I don't think this can be seen as evidence of a "dark side".
DiNicolantonio is an oddity. How does a 2010 Pharmacy School grad go from being the pharmacist at Wegmans to an Associate Editor of BMJ's Open Heart journal and described as a "leading cardiovascular researcher" in one of their press releases? He does not appear to have ever conducted primary research in any field.
Still, I'm not really sure that his study is on par with some of the other overtly unethical examples.
Post a Comment
Comment Moderation is ON ... I will NOT be routinely reviewing or publishing comments at this time..