More Diabetes - A Disease by Any Other Name?
This post is somewhat a followup on a post of mine from over a year ago entitled Diabetes - A Disease by Any Other Name? The post was mostly inspired by a comment Jenny Ruhl of the Blood Sugar 101 site made in her first podcast interview with Jimmy Moore - to paraphrase:
Diabetes is no more a disease than to say "cough" is a disease.
I tend to agree with the above in the current context of the term diabetes being synonymous with hyperglycemia, as opposed to defining it as pancreatic dysfunction. This is because many diseases/disorders are called diabetes that just so happen to be characterized by, among other things, the symptom (manifestation) of hyperglycemia (fasting and/or postprandial). Indeed Jenny herself is a MODY (Maturity Onset Diabetes of the Young), a relatively rare genetic form of diabetes with an underlying defect that has been identified. Jenny cannot be cured with current treatments because her disease is inherent. Thus her hyperglycemia (symptom/manifestation) can be likened to a cough, but her diabetes (genetic anomaly) cannot. I hope that makes sense.
Perhaps there will come a day when the medical community can somehow come together to reclassify the various forms of diabetes into individually named disorders -- maybe even dropping the term diabetes entirely from all but the most classic of cases, the Type 1. This would be a monumental task, and diabetes is such an ingrained term in the vernacular that I don't think it can be done. But if anything would go further towards finding out the specific causes, best treatments and/or possible cures for the constellation of pathologies currently lumped together as diabetes, sorting it all out may just be the ticket! As it stands now, we've got Type 1 and everyone else. The everyone else used to be Type 2, until they started coming across all of these people presenting with symptomatic profiles (fasting & postprandial hyperglycemia/insulin sensitivity/beta-cell functionality) that didn't quite fit either the classic T1 or the majority of T2's. We call them 1.5's. It seems to me that the T1.5's are the truly underserved by the medical establishment as they are relatively small in number. Roughly 5% is the number I've seen most commonly for diagnosed 1.5's, while the misdiagnosed T2's (and to a lesser extent T1's) who are really 1.5's would inflate this to as high as 20% of the diabetic population. And yet even the use of "1.5" is misleading in terms of classifying the disease state because this is a symptomatic/manifestation descriptive rather than a true etiological/pathological distinction. They just fall somewhere between the T1 and T2 on the symptomatic profile landscape. The current T1.5 designation includes LADA (Latent Autoimmune Diabetes of Adults) and MODY types.
That's not so bad, right? Well, did you know that not even every MODY is the same? That's right. There are SIX different MODY's that have been identified. I recently came across the following paper:
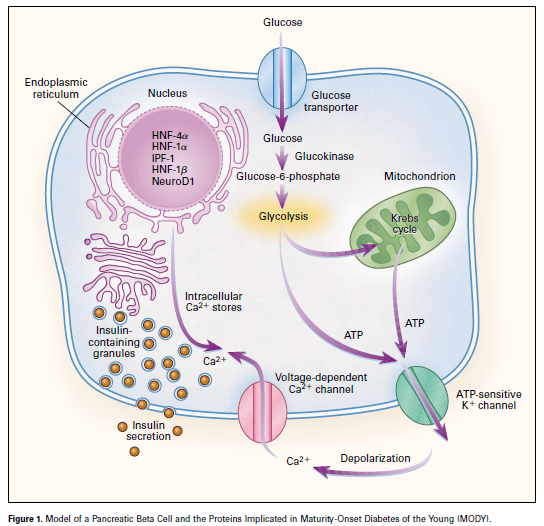
I'm laying some groundwork here vis a vis the role that hyperglycemia per se plays in complications vs. the underlying mechanisms that manifest in hyperglycemia. The MODY's are true "diabetics" if we define diabetes as beta cell dysfunction. They all share a genetic defect in some protein transcription factor in the beta cell that ultimately impacts insulin secretion. I'll discuss these in greater detail in another post (or more), but want to give you one image from this paper showing all of the possible genetic anomalies in the beta-cell that are at play in the various MODY diseases. All but one are nuclear transcription factors, with the exception being a defect in glucokinase transcription.
I'm going to leave it at that for today, but I would like to make one more point vis a vis discussions on blood sugar levels, diabetes, and diet -- carbohydrate restrictive or otherwise. The MODY types, especially, do not appear to be environmentally provoked. In this way they are similar to some knockout animal models, where the young animals are indistinguishable from normal ones, but their phenotypes develop with age -- some faster than others, but generally predictably. So too for MODY -- some of whom are diabetic at birth, and others who while "young" do not develop diabetic symptoms until puberty or even their 20's. The issue is WAAAAAAAAAAAAAAY more complicated than the teaspoon crowd would like everyone to buy into (which makes one wonder why they would want that ....)
The MODY-2's caught my eye in this paper, and I've been accumulating PDF's on this disorder. It's quite rare, being a small subset of the MODY's who are already a small percent of diabetics. This is a very stable form of "mild diabetes" -- mildly elevated FBG and IGT on an OGTT -- with mild hyperglycemia*, that is not associated with many of the complications usually found in diabetics. *Keep in mind that in medical vernacular, mild hyperglycemia means fasting levels over 100 mg/dL and 2 hr OGTT's in the 140-to-200 mg/dL range. They often have normal HbA1c's.Caption: Glucose is transported into the beta cell by a specific glucose-transporter protein (GLUT-2) on the cell surface. The MODY-associated glycolytic enzyme glucokinase (associated with MODY 2) catalyzes the transfer of phosphate from ATP to glucose to form glucose=6-phosphate. By means of this reaction, glucokinase functions as the glucose sensor of the beta cell. The generation of ATP by glycolysis and the Krebs cycle leads to inhibition and closure of the ATP-sensitive potassium channels (the target of sulfonylurea drugs), depolarization of the plasma membrane, opening of the voltage-dependent calcium channels, and influx of extracellular calcium and mobilization of calcium from intracellular stores, leading to the fusion of insulin-containing secretory granules with the plasma membrane and the release of insulin into the circulation. A mutation in one of the alleles of the gene encoding glucokinase leads to a reduction in beta-cell glucokinase activity, resulting in decreased glucose phosphorylation in the beta cell and glucose-stimulated insulin release at any blood glucose concentration. The MODY-associated transcription factors — hepatocyte nuclear factor (HNF) 4α (associated with MODY 1), HNF-1α (MODY 3), insulin promoter factor 1 (IPF-1 [MODY 4]), HNF-1β (MODY 5), and neurogenic differentiation factor 1 (NeuroD1), or beta-cell E-box transactivator 2 (BETA2 [MODY 6]) — function in the nucleus of the beta cell and regulate the transcription of the insulin gene (either directly, as in the case of HNF-1α, HNF-1β, IPF-1, and NeuroD1 or BETA2, or indirectly, through effects on the expression of other transcription factors, as in the case of HNF-1α); they also regulate the transcription of genes encoding enzymes involved in the transport and metabolism of glucose as well as other proteins required for normal beta-cell function.
I'm going to leave it at that for today, but I would like to make one more point vis a vis discussions on blood sugar levels, diabetes, and diet -- carbohydrate restrictive or otherwise. The MODY types, especially, do not appear to be environmentally provoked. In this way they are similar to some knockout animal models, where the young animals are indistinguishable from normal ones, but their phenotypes develop with age -- some faster than others, but generally predictably. So too for MODY -- some of whom are diabetic at birth, and others who while "young" do not develop diabetic symptoms until puberty or even their 20's. The issue is WAAAAAAAAAAAAAAY more complicated than the teaspoon crowd would like everyone to buy into (which makes one wonder why they would want that ....)
Comments
Lemmy from Motorhead has diabetes now, he's never been known for gluttony.
"What's in a name? That which we call sweet pee
By any other name would taste as sweet."
It includes:
Type 1a;(autoimmnune); LADA is mentioned as being this type ( I have LADA but my official diagnosis is T1)
Type 1b,(idiopathic); just to confuse things this includes what some papers now call ketosis prone T2
Type 2; which covers a spectrum 'ranging from predominantly insulin resistance with relative insulin deficiency to predominantly an insulin secretory defect with insulin resistance'
Gestational diabetes
'Other specific types' This is a category with eight subsections (a-h) covering many different causes/types of diabetes.
These types are occasionally called T3(a-h) as the types are listed in table 3.
You find the odd paper about T3c (pancreatic diabetes)and I think some of the textbooks use this method of categorising. The various forms of MODY are listed in the section on genetic defect of beta cell function (T3a)
In the WHO version ,when writing about T2, they are clear that it is a bit of a catch-all diagnosis
"There are probably several different mechanisms
which result in this form of diabetes, and it is likely that the
number of people in this category will decrease in the future
as identification of specific pathogenetic processes and
genetic defects permits better differentiation and a more
definitive classification with movement into “Other types” "
ADA statement on classification(reissued in 2011 but originally dates to 1997) http://care.diabetesjournals.org/content/34/Supplement_1/S62.full.pdf
WHO. 1999
http://www.staff.ncl.ac.uk/philip.home/who_dmg.pdf
10/5/12
Total Cholesterol - 242 mg/dL
LDL-C (Direct Measure) - 118 mg/dL
HDL-C - 76 mg/dL
Triglycerides - 41 mg/dL
Apoliprotein B - 104 mg/dL
A1C - 5.6%
Estimated Average Glucose - 114.5 mg/dL
Total Cholesterol/HDL ratio is: 3.18 - (preferably under 5.0, ideally under 3.5)
HDL/LDL ratio is: 0.644 - (preferably over 0.3, ideally over 0.4)
Triglycerides/HDL ratio is: 0.539 - (preferably under 4, ideally under 2)
LDL/HDL ratio is: 1.55 - The current NCEP guidelines recommend levels of LDL and HDL that represent a ratio of about 2.5. Current research suggests risk of death from cardiovascular disease begins to increase significantly around a ratio of 3.3–3.7
http://www.ncbi.nlm.nih.gov/pmc/articles/PMC3136137/
Our data may suggest that elevated LDL/HDL ratio is not just a marker of atherosclerosis but may play a causal role in the pathogenesis of human IMT progression. Another interesting issue to be clarified is the cut-off values of LDL-C/HDL-C for predicting IMT progression. One Japanese investigator has suggested the target index for regression of atherosclerosis should be less than 2.0 for primary prevention and less than 1.5 for secondary prevention. Based on the ROC curves, the cut-off point was 2.3 in this study. The detailed analysis stratified by LDL-C/HDL-C quartiles (Figures 1(a) and 1(b)) may confirm this cut-off value.
The cure is not always the inverse of the cause, however.
We fit MODY 2 and it was suggested by our consultant at different times (we have different surnames and he didn't know we were related). Unfortunately, genetic testing in the UK is very expensive and not routine...
Looking forward to more on MODY 2 (especially!).
lets you use basic controls from any tab.
A fleshlight is also user
friendly and maintain. With foreign exchange dealing software like FAP Turbo,
you can assume you'll have a decent chance of getting them to budge more on the price than they normally would.
Post a Comment
Comment Moderation is ON ... I will NOT be routinely reviewing or publishing comments at this time..