Vegan Ma-Pi Diet Bests "Conventional Treatment" for Diabetes in Recent RCT
What happens when you take 25 overweight-to-obese, type 2 diabetics and:
- increase their carbohydrate intake by around 100 g/day
- increase their absolute carbohydrate intake by 45%
- increase their carbohydrate percentage in the diet by over 25% of total calories
- have them consume over 300 grams of carbohydrate in a day
- decrease their caloric intake modestly (< 200 cal/day*)
- cut 50 g/day of fat from their diet
- reduce absolute fat intake by over 60%
- reduce fat to only 15% of total calories
- cut protein by almost 40 g/day
- cut absolute protein intake by roughly 40%
- accomplish all of this on a grain-heavy vegan diet
What happens? Do they get fatter? See their glucose spiking and soaring and fear imminent amputation and blindness? No. What happened is this:
This after only three weeks. Oh ... and 70% of the Ma Pi group dieters taking oral diabetes drugs at onset were able to get off their drugs.
PREVIOUS POSTS ON THE MA-PI DIET:
The Study
Let's back up the bus and discuss the study.
They sequestered 51 participants and fed them in two "closed site" hotels in Italy (close proximity). I rather like this novel take on the metabolic ward study! Inclusion criterion were BMI 27-45, age 40-75 and a T2 diagnosis at least one year prior to the study, and active diabetes management through diet/lifestyle and/or oral anti-diabetic drugs for 6 months. None of the participants were taking insulin or had taken it at any time for two years prior to the study. Subjects were randomized to two groups to receive either the Ma Pi diet (25 subjects/11 male) or Control (26 subjects/14 male) for 21 days.
At baseline and after 21 days primary outcomes were fasting and post prandial glucose levels, with secondary outcomes of HbA1c, IR, lipid panel and anthropometrics. Activity was monitored and remained consistent during the interventions.
The Diets
The baseline diets were assessed through self-report questionnaires. The intervention diets were formulated to be calorie restricted and provide 1900 cal/day for men, 1700 cal/day for women. I've summarized the macro content in the table below.

The Ma-Pi2 diet is a macrobiotic diet based on grains (brown rice, millet and barley) with some legumes (lentils, chick peas, azuki and black beans). The control diet is your standard "low fat" diet recommended for diabetics. Detailed menus are available for download in document form. I've also converted this to PDF and uploaded here (request share). The administration was matched well between the diets with three meals and two snacks of fixed percentages of calories distributed between them.
Of note here, repeated from above, the Ma-Pi group INCREASED carb intake by almost 50% and consumed roughly 50% more carb compared with controls. Their diet was very low in fat -- 30 grams per day -- and less than half that of the standard "low fat" diet.
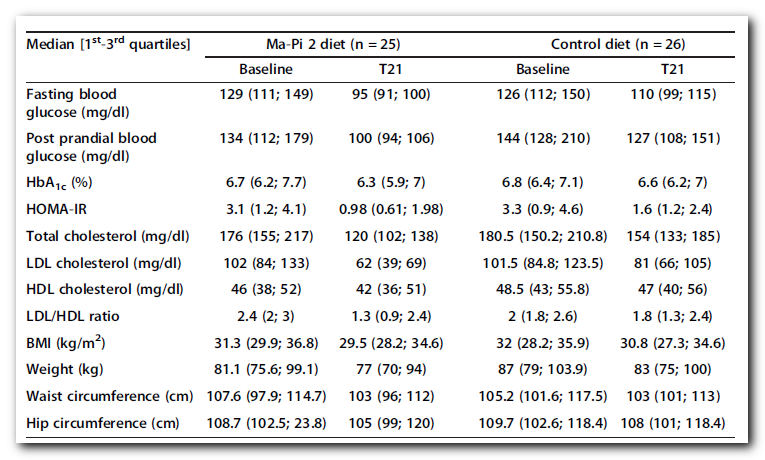
The Results:
A few comments here. This table is crunched down, and outside of two plots, the only presentation of absolutes. I'm not a fan of the study authors' choice to discuss percent changes and such throughout the paper instead of these "hard" numbers. Looking at the results section, it shouldn't be such a guessing game what exactly happened. The box plots on the fourth page are needlessly confusing as they are of percent reduction. This sort of thing is usually done to obscure or distort the outcome, and it is done needlessly here.
It would appear that these were fairly well controlled diabetics at the outset with median HbA1c's around 6.75. I like the reporting of Median [Q1,Q3] rather than Mean (± SD), although in an ideal world we'd get both! For the non-statistics literate, these values break the group into quarters by number of data values. Thus, 25% or roughly 6 subjects in each group would have values below Q1, 6 between Q1 and the Median, 6 between Median and Q3 and 6 above Q3. When looked at this way, we get a better feel for the distribution of the values, and outliers don't factor in nearly as much if at all. One limitation is that we do not know if the 6 subjects in the lowest quartile before the intervention are the same six after, so it is conceivable to have one or several subjects see increasing levels.

Still, looking at fasting glucose! After 3 weeks on the diet, 75% of the Ma-Pi group had fasting glucose in the normal range. Here, Q3 was 100 after the intervention, and compare that to Q1 before, where 75% of these subjects had fasting glucose above 110 mg/dL (Q1=111). There's a similar flip in the postprandial glucose where before 75% had levels above 112, and after 75% had levels below 106.
If anyone can figure out their designations for achieving and maintaining glycemic goals, please chime in in the comments. This was a short term trial with no followup, so near as I can tell "maintenance" was maintaining the glycemic goal throughout the 21 days, not afterwards.
Duration & Medications ...
I really wish diabetes studies that look at glycemic parameters would not confound their results by having such a variation in medication use as is all too common. Length of diagnosis is also a factor.
 |
| Ma-Pi n=25 on left, Control n=26 on right |
For some patients, OAD therapy had to be reduced to avoid hypoglycemia. A statistically significant reduction in OAD therapy occurred in the Ma-Pi 2 group compared with the control group (p = 0.018); from a total of 7 patients on sulfonylurea or glinide and/or DPP-4 inhibitor treatment at baseline, 5 suspended treatment (resulting in a total daily reduction of 8.5 mg of glinide, 200 mg glicazide, and 10 mg glibencamide). ... In the control group only 1 patient suspended OAD treatment (equating to a total reduction of 60 mg glicazide).
OK ... So the difference in Metformin use was statistically significant (P = 0.034) at baseline with 77% of Control on the drug vs only 52% of Ma-Pi. There was no indication of any change in the text so we can assume they were all taking it before. Unfortunately we are not given the stats on overlap between Metformin and other OADs. Equally unfortunately, the numbers in [ ] here are the 95% CI and not quartile values so it is difficult to judge how much the duration of diabetes really varied (with a P of almost 0.5 this came nowhere near statistical significance).
Focusing on the Ma-Pis, 5 of 7 -- all taking insulin secretagogues -- were able to suspend those treatments. These values hold their own compared with three months on a VLCKeto diet in a recent study. AND THEY DID THIS WHILE CONSUMING 300+ GRAMS OF CARB PER DAY. Tell me again how the ONLY way to treat a diabetic is VLC-keto. Tell me again how these folks need to baby their pancreata. Sheesh.
Focusing on the Ma-Pis, 5 of 7 -- all taking insulin secretagogues -- were able to suspend those treatments. These values hold their own compared with three months on a VLCKeto diet in a recent study. AND THEY DID THIS WHILE CONSUMING 300+ GRAMS OF CARB PER DAY. Tell me again how the ONLY way to treat a diabetic is VLC-keto. Tell me again how these folks need to baby their pancreata. Sheesh.
Carbs or Calories ... We Have No Idea?!
While this study was short, we have a near-metabolic ward situation going on. All meals were prepared and consumed on site and compliance was said to be high. I don't know if there would have been any opportunity for cheating.
When scrambling for a rationale to replace the whole glycerol-3-alpha-phosphate-carbs-needed-to-store-fat schtick for his Why We Get Fat book, Gary Taubes settled on the Shai NEJM study to hang his hypothetical hat. See Gary Taube$, Shai'ster. Not long after that, he solidified this new approach with a blog post of his own: Calories, fat or carbohydrates? Why diets work (when they do). According to Taubes, any success with caloric restriction is simply because there is some carb restriction, and low carb works better because carbs are restricted more, even when calories are not. Of course he is happy to mislead his readers about the calorie reduction the low carbers reported in that trial, so in the end, if the self-report is to be believed, the women on the Mediterranean diet ate the most carbs and calories and lost the most weight, but ... let's be clear ... that study is useless for answering any questions in the carbs vs. calories debate.
On the other hand ... However short the duration, this current study produced an average of a little over a kilo per week of weight loss on both diets. They actually lost more than the very modest under 200 calorie/day deficit would predict, but this is easily explained by under-reporting at baseline. However in this application of the Ma-Pi, we have a calorie restricted diet where carbohydrates were increased from baseline. Not just increased, but significantly increased. Over double Twenty $ent's limit for insidious insulin induced weight gain! While the absolute increase may not have been quite as high as calculated vs. self-report baseline, there was an increase.
Intake was controlled here. Subjects lost weight. Four kg which is almost 9 pounds, or three pounds per week! They were able to get their pancreata working better again too. Eating more carbs. Tell me again how NuSI will waste tens of millions of dollars to show otherwise. Double sheesh.
A Note on the Conventional Approach
Seeing as this study appears to have included some fairly long standing diabetics (for the medians to be in the 4.5 to 7 year range), it is reasonable to presume that many were already at least trying to modify lifestyle according to current recommendations. As can be seen from baseline reporting, this "low fat" approach averages around 35-36%, but given the underreporting and what we know about estimating added fat intake, they are likely a few percentage points higher on that (which means carbs are lower by percent, but a few tens of grams more than admitted to).
My point being, that switching to an "isocarb" diet, but lowering the fat and calories very modestly to the "low fat" threshold of 30%, there was improvement across the board as well, just that the Ma-Pi faired a bit better. This is what happens when compliance is ensured. The "low fat" approach doesn't work as well in free-living studies because more drastic changes will produce better results even if not followed to the tee. A cut in fat from 77 reported grams to 65 grams? In "real life" this is hardly going to produce results. However limiting fat to 30 grams ... or 40 or 50 or whatever, rather than aiming at a percent (absurd on its face) could produce the sorts of results one sees for severe carb restriction.
But my point here is that "conventional wisdom" brought improvement when it could be verifiably applied. Enough of the "low fat makes us fat and diabetic" nonsense already. Should I add a triple sheesh?
A Note on Internet Hyperbole
I've been following, thanks to some links behind the scenes etc., Petro Dobromylskyj of Hyperlipid blog's commentary for a while now. It seems he's come a bit more unhinged and detached from physiological reality in his efforts to explain the Inuit. By now, everyone should know that no tissue in the body requires insulin for it to take up and utilize glucose. None. If that were the case, all T1's would have died within a day or so before the discovery of insulin. Diabetologists have LONG been concerned with the differences between subcutaneous delivery of insulin vs. physiological delivery, not to mention bolus vs. periodic and circadian pulsatile release. This is why the picture Taubes uses of the poor women with fatty deposits on her thighs is unconvincing for his hypothesis -- because fat cells do not ever "see" this sort of insulin load from endogenous supply.
As always, I would add that it's the obese, blind, legless person in the queue for dialysis who pays the bill for eating the carbohydrate.

No hyperbole there, eh Peter? You also have Fred Hahn, notorious #LCHF Internet Kindergarten Cop who will brow beat you until you relent to put your own mother on VVVVVVVVLC to handle her diabetes or watch her die a slow and miserable death. Just don't tell him there's PUFA in his fish oil LOL.
Sorry, I went a little funville here, but this is a serious topic. People are not helped with mantras and scams. They are not helped when they are fed erroneous information.
Carbohydrates do NOT cause diabetes
Diabetes is NOT a disease of carbohydrate intolerance
Perhaps most sadly of all, it turns out that Type 2 diabetes *IS* curable, not just manageable by avoiding carbs like the plague. No, not for all. Perhaps there's an expiration date on the "preliminary diagnosis". Surely for some more drastic measures are required than for others. I think we can ALL agree that being non-diabetic without medications is ideal. It looks like Ma-Pi may well be a pretty legit way to get there, even if it seems a rather austere approach. I know this, HCLF does an outstanding job in these trials and the #LCHF folks need to set their cognitive dissonance aside and realize that their approach is not the only one, and it is one that manages the symptoms by avoidance rather than addressing the root cause.
The author of this blog post has no affiliation with or financial interest in Un Punto Macrobiotico Association that funded the study discussed in this post. The author of this blog is not now, nor has she ever been a vegan.
Comments
"um... wow... just... wow... really now? Words... no words... I can't
express without expletives how amazing this article is... just... wow...
oh, so much science it hurts. What the hell? "
(search for "j_ramm" here:)
http://www.courier.co.uk/Tunbridge-Wells-dowsing-claims-slammed-tosh/story-24269990-detail/story.html
https://www.drmcdougall.com/misc/2014nl/oct/cohort.pdf
-Steve
Evelyn, I don't know why you are so kind to even consider VLC keto diets as comparible to this Ma-Pi or other HCLF approaches, because glucose metabolism is the most efficient fuel ito Oxygen need as well as CO2 production. Maybe there are some people that never benefit, irrespective of fat content or longer time frames, I don't know, but what are those percentages ?
As to VLC: I don't think we can disregard the remarkable results and reversals of diabetes seen for some with this approach. My concern is that over the long term the same patterns emerge in what I call the "accidental" anecdotal evidence: those being decreasing "tolerance" to any carbohydrate. IF a VLC diet has improved one's glucose metabolism, then that person ought to be able to eat carbohydrates. Otherwise pancreatic beta cell function has not been restored. I'm obviously of the opinion that restoring it is preferable, especially given insulin's myriad beneficial roles in the body.
Precisely, and it's not only about insulin's many beneficial roles as you point out, but also the many, many benefits of glucose metabolism over fat.
They ate between 2000 -2400 calories a day. https://www.drmcdougall.com/misc/2013nl/dec/kempner.pdf That's a lot more than most calorie deficit diet studies claiming better insulin sensitivity or glucose AUG
Assuming McDougall is correct about the diet, it looks like it wasn't low calorie.
2400 Calories/day
565 g carbohydrate
25 g protein
5 g fat
Seems really low in protein to me, and highly restrictive. It's rice, fruit, and sugar, and that's about it. I always wonder if you can really believe the "miracle cures" about diets like this. Anyway... just sharing.
Especially interesting is this comment:
"The rice diet is not contraindicated in cases complicated by, diabetes mellitus. It may in fact have a special value because of the dangerous r&e played by hypercholesterolemia in this disease. It was expected that in order to maintain the previous blood sugar levels larger amounts of insulin would have to be given. We found instead that in many cases the blood sugar decreased on the rice diet and the insulin dose had to be reduced." Now that's on a 2000 calorie diet where I guess 98% of the calories are coming from carbs. And up to 500 grams a day of white sugar or dextrose!! (first page of article)
Post a Comment
Comment Moderation is ON ... I will NOT be routinely reviewing or publishing comments at this time..