Cholesterol or Inflammation?
I wanted to share this study with my blog readers that I had found and shared a bit of on Twitter a little while ago. This has been prompted by ongoing discussions there and elsewhere on social media regarding blood lipids. By "cholesterol" I am of course using the general term that in today's terms refers mostly to the low density lipoproteins or LDL.
C-Reactive Protein
A Simple Test to Help Predict Risk of Heart Attack and Stroke
This is not so much a study as a communication. It is also on the "Cardiology Patient Page" of the journal Circulation, and as such quite readable. I'd suggest any and all interested do so as I don't really have the time to go in depth into the entire thing.
A key issue with the Jimmy Moore/Eric Westman book Cholesterol Clarity, that has been exhumed once again by Nina Teicholz, and even a Peter Attia appearance on the Dr. Oz show, is the Ronald Krauss driven idea that LDL-C doesn't matter, it's the particle size. Over the years I've heard "large fluffy" LDL described as anything from not-as-bad (Krauss' current descriptive) to protective, where the latter designation is clearly erroneous. It is fairly widely accepted that particle number is an important predictor, and the issue of particle size comes in when you have normal concentration carried by a large number of particles (bad) vs. slightly high concentration but carried by a small number of large particles (not so bad). Thomas Dayspring and others have made it clear that when your cholesterol is very high, size doesn't matter and all the fancy testing is unnecessary -- you are at higher risk. I discussed this here: When Size Matters (and when it doesn't) .
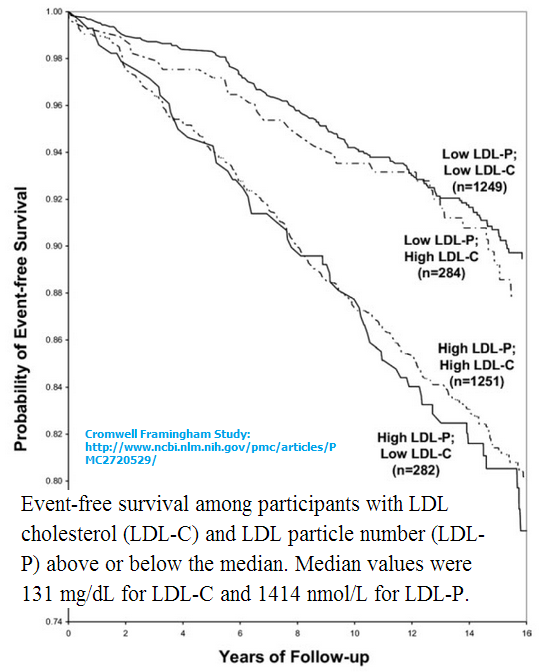 Here's the pretty famous image demonstrating this. Note that Low vs. High designations are for below or above the median, and sadly many insisting that LDL is entirely meaningless often fall quite well above the median -- like up in the 90-some percentiles!
Here's the pretty famous image demonstrating this. Note that Low vs. High designations are for below or above the median, and sadly many insisting that LDL is entirely meaningless often fall quite well above the median -- like up in the 90-some percentiles!
Another buzzword that has taken hold in the IHC is inflammation. What is inflammation? Is it a physical manifestation, or is it some markers that have been designated under what has become a rather broad term? It is a common mantra these days to dismiss all potential bad-news-LDL on the basis of "I have no inflammation so it won't rupture". I'm can't help but think of Dreamfields pasta and all the low carbers who would consume it when the manufacturer told them it had carbs in it, they were just "protected". Consumers were given specific cooking instructions (hope you like your pasta al dente!) and to cook only what you planned to eat right then. Reheating is out of the question. I don't know about you, but I'd rather not eat the carbs in the first place than worry over whether they would be released in my digestive tract, and I pretty much feel the same way about atherosclerotic plaques. No, that the Masai had them and didn't have high incidence of heart attacks is of no relevance here ... unless you are a Masai living the warrior lifestyle.
The gold-standard measure of inflammation at the current time is C-reactive protein or CRP for short. In some studies CRP is improved with low carb, in others, like the one blogged on here, it is increased. Still, there's a false sense of security being established out there by the advocates of low carb diets, that so long as CRP is low, everything is A-OK. Mind you, the best you'll get from an expert if you corner them is "well we really don't know" -- but this hasn't stopped folks like Jimmy Moore from making wild health claims regarding their stellar lipids (I can think of another term deriving from stars that is more appropriate). It is one thing if he, or you or anyone else wants to take a risk based on the evidence in hand. It is quite another to be making these claims and the words I'd use to describe this range from irresponsible to downright criminal. Always keep in mind that anyone can say pretty much anything in a book these days so long as they put a medical disclaimer in there. There is no filter, and even esteemed publishing houses see fit to publish anything without technical or factual review.
So, the paper:
Why Do I Need Both CRP and Cholesterol Measured?
Both cholesterol and CRP predict risk, but you cannot predict your CRP level on the basis of your cholesterol level (or vice versa). That is because each of these blood tests picks up a different component of the disease process. This independent and additive effect is demonstrated in Figure 1, which shows cardiovascular event-free survival for initially healthy individuals according to levels of both CRP and the so-called “bad cholesterol” or LDL cholesterol.

The article goes on to discuss how CRP is a better single predictor. Consider this, however. This is "at baseline", not from birth. So what this may well indicate is that the inflammation follows the buildup (and that makes common sense). In other words, those with high CRP at baseline were already in the early stages of disease manifestation so it is no wonder they were more likely to develop advanced disease. It would be very interesting to see such an analysis with particle numbers instead of just the LDL-C if such data is available.
But clearly, the Low CRP/High LDL are pretty close to the High CRP/Low LDL right there in the middle of the pack. This is "high" as in above the middle, not as in some of the familial hypercholesterolemia-like LDL levels some sport proudly. It is not a stretch to consider that such a line for those types might end somewhere in the lower quarter of this graph.
To me the bottom line is that we are in uncharted territory with the lipids produced on extreme diets -- and anything much over say 40-45% fat in content is pretty extreme for the vast, vast, vast majority of humans on the planet. I don't think it is scare mongering to point this out and caution my readers about the health advice being doled out in low carb circles.
Comments
When my hypothyroidism went undiagnosed for a few years, my LDL went up. After diagnosis and hypo treatment, it went down very slowly. When it was still high, my endo did the VAP test on particle size, and I was happy that it showed I had 100% of the large, fluffy kind which I'd been brainwashed (by low carb advocates) into believing was good.
My cardiologist told me that was nonsense and that particle size is basically irrelevant. The notion that it's important persists in low carb circles and people are encouraged to ignore high LDL levels.
Also, I initially bought into the 'coconut oil' is magnificent view, but fortunately because of my hypo, I get blood tests every 4 months, including a lipid panel. The wonderful coconut oil raised my LDL by 40 points in one 4 month span! My endo asked about any 'dietary changes' I'd made, and I immediately thought of the CO--and stopped using it. On my next labs 4 months later, my LDL was down those 40 points. It was definitely the CO.
And I only eat low to moderate fat--not the high fat of most low carb crazies.
Since few of them are regularly tested as I am, I can only imagine (in horror) the damage they may be doing to their bodies by believing all the crap that Jimmy and his pals promote.
I was pretty floored that Westman collaborated with Jimmy in the first place, but hoped he might serve as a moderating voice in that book. He wasn't. Mostly his doctor's notes range from the inane (eggs are just like whole baby chickens!) to chant-like. There is a section at the end of the book where Jimmy diagnoses peoples lipid panels and includes his own. The sole factors used for health vs. risk were HDL and trigs and Jimmy's own lipids put him in the healthy category.
Which Micro- & Macronutrients Intakes Are Associated With High HDL Levels? Study Shows Magnesium & Folate Are, High Carbohydrate & Total Animal Fat Intakes Are Not!
http://www.nutritionandmetabolism.com/content/pdf/1743-7075-11-44.pdf
Effects of dietary components on high-density lipoprotein measures in a cohort of 1,566 participants
http://download.thelancet.com/images/journalimages/0140-6736/PIIS0140673614610096.gr3.lrg.gif
The Atkins Diet raises CRP during weight maintenance while the Ornish Diet lowers it:
http://www.andjrnl.org/article/S0002-8223(08)02336-5/pdf
Same thing more or less, but during weight loss:
http://www.ncbi.nlm.nih.gov/pubmed/17536128
Red and processed meat consumption associated with higher CRP:
http://www.ncbi.nlm.nih.gov/pubmed/19074209
http://www.ncbi.nlm.nih.gov/pubmed/22596177
http://www.fasebj.org/content/28/1_Supplement/628.21
Medications - 10mgs/day Atorvastatin, 120mgs/day Armour Thyroid, 100mgs Testosterone Cypionate 2x/week PLUS a boat load of supplements
Fasting Glucose - 83 mgs/dl
HA1C - 5.7%
Serum Insulin - 4 Micro IU/ML
HS-CRP - 0.9 mg/l
LDL Particle Number - 1011 nmol/l
Small LDL - 184 nmol/l
Medium LDL - 167 nmol/l
HDL Large 5946 nmol/l Reference Range 4334-10815
LDL Pattern - B
LDL Peak Size 208.5 Angstrom Reference >OR = 218.2
TC - 120 mg/dl
HDL - 54 mg/dl
LDL (Calculated) 56 mg/dl
Triglycerides - 50 mg/dl
Non-HDL Cholesterol - 66 mg/dl
Cholesterol/HDL Ratio 2.2
Apo A1 - 138 mg/dl Reference Range 94-176
Apo B - 59 mg/dl Reference Range 52-109
ApoB/A1 Ratio - 0.41
Reference Range
Below Average Risk - <0.29
Average Risk - 0.29-1.30
Above Average Risk - >1.30
Homocysteine, Serum 9.9 umol/l Reference Range <11.4
LP-PLA2 250 ng/dl Reference Range 81-259
Liproprotein A <10 nmol/l Reference RAnge <75
Adiponectin 7 mcg/ml
Vitamin D, 25-OH, Total 74 ng/mL
CoEnzyme Q10 - 1.14 mg/L Reference Range 0.44-1.64
Therapeutic Range Recommended for CVD >2.50 mg/L
I provided some papers on the benefits of pescetarian dietary changes, However, as far as 'enjoy the red meat and butter' spiel went. Yeah, the plant-based offerings were the overall winner. The narrative seemed clear: Want low lipids and low inflammation, then centre the diet around plants.
And that's the interesting thing. Aside from the outright anti-cultural quacks, one would be hard-pressed to find a vegetarian or vegan diet-advocating doctor, living in blatant denial of the basic reference range for cardio-metabolic markers. Despite their near-reductive fixation on cholesterol, they're not telling their patients to ignore their inflammation, glucose and lipid markers, but rather the opposite, as they're showing off results on these very wide-ranging parameters.
What happens after is a matter of who's selling what and how many people within the circle jerk can support their product and create the illusion of 'perfection' through disingenuous reviews.
This bears repeating. The burden on the low carb advocates is high for many reasons not the least of which being they often counsel against those markers that are inconvenient.
I don't have the time today to track this down but I plan to.
Embracing Fat for a Healthy Heart Is a Notion Based on Flawed Science
BY DEAN ORNISH, MD
"My recent heart scan results were 50% lower (= better) than predicted. Apparently I am doing something right.
You might think that my lipid values would reflect that. Not quite. They were measured twice in the last two weeks, first with a Cholestech LDX machine (instant results); second, ordinary lab tests.
Here are the scores (first test, second test). Total Cholesterol: 210, 214, which is “borderline high” (borderline bad) according to the Cholestech LDX quick reference sheet. HDL = 17, 36, which is “low” (bad). TRG = 62, 75, which is “normal”. LDL = 180, 163, which is “high” (bad).
There is no hint in these numbers that I am doing the right thing! If anything, they imply the opposite, that I’m doing the wrong thing. This supports all those people, such as Uffe Ravnskov, who say the connection between cholesterol and heart disease is badly overstated."
http://www.ncbi.nlm.nih.gov/pmc/articles/PMC2720529/
LDL Particle Number and Risk of Future
Cardiovascular Disease in the Framingham Offspring Study – Implications
for LDL Management
Conclusions
Among alternative measures of LDL in this large, community-based study, LDL
particle number was more strongly related to incident CVD events than LDL-C. Of particular relevance to the use of specific LDL treatment targets as indicators of the adequacy of LDL lowering therapy was the finding that low LDL particle number was a better index of low CVD risk than low LDL-C. Non-HDL-C provided risk prediction intermediate between LDL particle number and LDL-C, with evidence suggesting that the better prediction relative to LDL-C was due less to non-HDL-C including atherogenic triglyceride-rich particles (VLDL and remnants) and more to its strong correlation with LDL particle number. Finally, our novel
finding that LDL particles are more cholesterol-depleted when LDL concentrations are lower, independent of triglycerides or LDL particle size, helps to explain why patients with low LDL-C often have disproportionately higher numbers of LDL particles (7–13). Our data show that persons with this LDL disconnect have higher CVD risk. It is therefore reasonable to anticipate that such discordant
individuals would derive clinical benefit from more intensive LDL lowering than would have been indicated by their LDL-C level. Data from statin intervention trials are needed to test this hypothesis.
But the real upshot from your blood lab is your high-normal LP-PLA2 and moderately high Homocysteine and CRP, despite having very low LDL-C and moderate LDL-P. Do you know your MTHFR status? Take B vitamins? You have some good numbers but your risk is not as low as they should be because of what might be endothelial inflammation -- that's probably why your CRP is 0.9. For someone like you, its should be 0.1. You have some inflammation but it's not metabolic and it could be genetic, autoimmune, or drug induced. Did you have your spleen removed?
He misinterprets both the CAC test when it's subclinical (soft plaques) and the 50% change which he attributes to amelioration. Those numbers are meaningless unless you're old and should be interpreted as either / or. When you're in your low 50s and it's not zero, it indicates some problems. It should be zero if you're under 50. But the non-zero numbers themselves are meaningless. Then he misinterprets TC going up from 210 to 214 as bad, when it is achieved through higher HDL and an improved Framingham ratio: TC / HDL. His low trigs are not gonna save the day when his numbers are that bad. This is the health guru that Paleo looked up to? This is just so sad. And the best he can do is backslap Uffe Ravsnkov in his ignorant bliss.
Did you review Keto Clarity as well?
Cheers for linking. I saw the comments and the usual circle-jerk response.
I think that the Amazon review system is open to abuse. Both in terms of cabals of individuals (with mutual interest) reviewing each others products and creating this false illusion of perfection. Hence circle jerk. This is followed by basically ganging up on and down-voting any dissenting opinions and when that fails, even manipulating Amazon's administration into deleting the dissenting opinions.
It seems like that the NuttyK crowd was behind the removal of some of these reviews.
SO - 12/24/2013
WBC - 4.3 THOUS/MCL Ref Range 3.8-10.8
RBC - 5.14 MILL/MCL Ref Range 4.20-5.80
Hemoglobin - 17.3 G/DL Ref Range 13.2-17.1
Ferritin not tested - will have that done next time
APOE - 3/3
MTHFR status
C677T - +/-
A1298C - +/-
SO - I take Jarrow B Right which contains 400 mcg of Quatrefolic
My hsCRP declined from 3.0 to 0.0 in the last 6 months - maybe because I started taking 3 grams of fish oil/day
Still have my spleen
The high LP-PLA2 is of concern - any ideas as to how it could be lowered?
Thanks, all.
I posted a pretty long comment yesterday and I dunnoe know if it went into spam or got removed, it seems comments that are submitted after me are posted already, but mine is nowhere to be seen. If you don't want to entertain my comment, can you at least approve it to be posted and I am sure your readers can chip in. As far as I am aware, my comment was civil and relevant to the topic of your post. I would really appreciate, if you could do that, thank you.
Fish oil is anti-inflammatory if you believe in n6-n3 theory, which is not proven. How are your liver enzymes: ALT/AST should be in the teens if you have no metabolic inflammation. Your Albumin should be >= 5, your Globulin I bet is right around 2, low normal, given your 4ish WBCs. For Homocysteine, >13 could be problematic and maybe 6-8, 6-9 are optimal. Your TSH/FT3 ok since taking Armour? See any bump up in WBCs after taking it? I'd ask for ANA and ESR next time.
10/22/13
AST - 21 Ref Range 10-35
ALT - 26 Ref Range 9-46
Albumin - 4.3 Ref Range 3.6-5.1
Globulin, Calculated - 2.4 Ref Range 1.9-3.7
A/G Ratio - 1.8 Ref Range 1.0-2.5
12/24/13 - will have these retested in Dec
TSH - 1.62 Ref Range 0.40-4.50
T4, Free - 1.4 Ref Range 0.8-1.8
T3, Free - 3.1 Ref Range 2.3-4.2
T3, Reverse - 40 (High) Ref Range 8-25
I interpreted that as Dr. Attia agreeing to the large number of LDL particles causing endothelial damage as opposed to strictly based on size. Or perhaps he was too mesmerized by Dr. Oz's "weekday afternoon residency at the Golden Nugget" style of TV theatrics to clarify?
First, the visual is inescapable. You have your single bouncy ball that rolls along, and then a ton of small balls which he then uses to tear up the vessel wall.
At around 2:45 Oz says:
Once it gets into your blood, if it's in a BIG form of cholesterol like this, this cholesterol rolls through your artery represented by this, and without any problem flows out of your body, or where it needs to go.
Attia looks along with dumb look on face. Speak up man. Nah. It's national TV exposure.
I read one of your references and had intended to read the full text before responding -- the one with the reduction of risk with age. Could that be interpreted as the more vulnerable having already died off? I didn't have a chance to look closely enough.
One of the issues with saturated fats is that one way they raise LDL levels is via the cholesterol receptor.
I have been sent a number of additional references on this topic and many still point to LDL *per se* remaining a good predictor of CVD. Take that to LDL-P or apo-B (associated with LDL) and the predictiveness strengthens. Is it the LDL or some underlying metabolic milieu that causes it? That's what folks continue to try to sort out. For now I'd hedge my bets carefully and think it is irresponsible of those who promote the notion that LDL is meaningless.
Again, my apologies for not responding sooner.
FIrst of all, I have to clarify that my dietary approach is very moderate (neither low carb., low fat nor high fat) and I am not saying that LDL level is totally meaningless (I think context matters ), but I definitely disagree with the rather reductionistic view of the correlation btw. LDL and CHD. I subscribe to the oxidized LDL (oxLDL) hypothesis, so I am aware that high LDL will inevitably lead to high oxLDL, but the cut-off point would be 6.0 mmol/L. My view is that, in the high fat, low carb (HFLC) circles, most of them do not believe in CICO, hence in their hypercaloric and high fat context, all of that fat must go somewhere, hence hypercholesterolaemic-like LDL level, so it is unfair to blame satfat in this context.
Regarding saturated fat, I think in the context of a moderate fat intake, the downregulation of cholesterol receptor is balanced by the reduced susceptibility of LDL to oxidation. Furthermore, prospective studies seem to show there is no benefit to satfat reduction in the long-term. On the other hand, the upregulation of cholesterol receptor with PUFA could very well be a physiological response to elevated oxLDL.
If I harken back to my days at Paleo Hacks I'm reminded of so many who saw their lipids soar when adopting the high "paleo fat" diet -- coconut oil and butter. How butter became paleo is beyond me, but these high sat fat fats almost invariably threw lipids outta whack. All LDL-receptor mediated? I don't know. But in LA Veterans they consumed 40% fat of mostly PUFA -- and crappy PUFA at that as rather than consuming different foods high in PUFA, they made the diet as similar to a regular one as possible with margarine, "filled milk" and the like. LDL went down.
I dunno. I would love to delve more deeply into this but it's not top of my list of interests at the moment. For me, a woman whose LDL has always been "a bit high" (as in borderline by the established ranges) with robust HDL (not out of the ordinary high either) resulting in a TC that has flirted with being higher than "optimal" since I was 19 and got my first TC test, I am more interested in changes than absolutes. If I adopted a diet and my LDL took off into FH ranges, I'd reverse course .... not write a book and take enough people out of context to convince myself that not only am I not taking risks with my health, but am somehow healthier with a whack lipid profile.
Thanks much for the studies. I hope to revisit them!
You have enough FT4 but your FT3 is "only" mid-normal but your RT3 is high. Naturopaths will interpret your blood work as if your FT3 is being siphoned off to RT3, and your FT3 should be in the upper quadrant. Your FT3/Rt3 is only 8, while it should be >10 or >20. This is all still crapshoot. If you have hypothyroid symptoms, then maybe that's happening. But the FT3/RT3 ratio and the FT3 level themselves defy interpretation and sometimes are symptomatic of generalized hormonal dysfunction, not just thyroid hormone dysfunction. That's why knowing your health history and whether you indeed were hypothyroid (based on TSH), have autoimmunity, i.e., Hashimoto's, are important. If you listen to naturopaths, the catch-all answer is thyroid, since all they know is the Ft3/Rt3 ratio. Are your symptoms being addressed sufficiently by Armour?
Post a Comment
Comment Moderation is ON ... I will NOT be routinely reviewing or publishing comments at this time..