Could Early Insulin Therapy for T2 be Coming to Canada?
A short post here, because I have no peer review study to refer to. But Nigel Kinbrum recently blogged on this media report: New treatment might put Type 2 diabetes in remission.
This report touted 75% remission from T2 using self-administered insulin of 4 injections per day for one month. This is less aggressive than reported in other studies (some summarized here, table below)
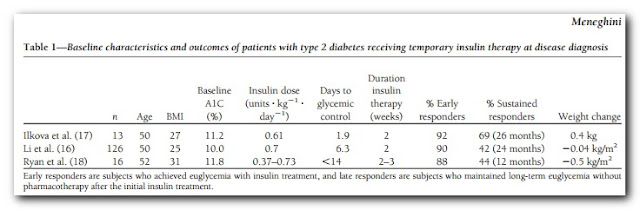
Most of these used insulin infusions for a couple of weeks and early response rate was around 90%. This treatment may be more practical (and cost effective?) but perhaps not intensive enough to to get the optimum outcome. Still, 75% is impressive. The article discusses that they want to follow up with an oral diabetic drug to "save" the pancreas, which the studies above involved lifestyle "treatment" only.
So this article is about a year old and I wondered if it ever made the literature. I did a PubMed on Dr. Bernard Zinman and got no love. But a Google Scholar search seems to indicate that Zinman is involved in establishing treatment protocols in Canada. Were I a diabetic or at risk in Canada, I would consider this very good news indeed. I would absolutely want to try to put my diabetes into remission and re-establish functional beta cells. If there are any Canadians in the audience, I'd appreciate if you have any info to add. For now this is just a "bookmark" of sorts.
Comments
Regards,
Rad
http://www.lunenfeld.ca/researchers/zinman
The paper:
Diabetes Obes Metab. 2012 Oct;14 Suppl 3:161-6. doi: 10.1111/j.1463-1326.2012.01658.x.
Short-term intensified insulin treatment in type 2 diabetes: long-term effects on β-cell function.
Retnakaran R, Zinman B.
Source
Leadership Sinai Centre for Diabetes, Mount Sinai Hospital, Toronto, Canada.
Abstract
The
natural history of type 2 diabetes (T2DM) is characterized by
progressive deterioration of pancreatic β-cell function, leading to
worsening glycemia over time. As current antidiabetic therapies have not
yet been shown to profoundly alter this natural history, many patients
ultimately will require exogenous insulin therapy to obtain adequate
glycemic control. Interestingly, the temporary use of short-term
intensive insulin therapy early in the course of T2DM has recently
emerged as a therapeutic option that may offer favourable long-term
effects on β-cell function. Indeed, after receiving this treatment, many
patients will experience sustained euglycemia without requiring any
antidiabetic therapy. This apparent 'remission' of diabetes is likely
secondary to improved β-cell function and can last for more than a year,
although it is not sustained and hyperglycemia eventually will return.
Nevertheless, owing to its effects on β-cell function, short-term
intensive insulin therapy holds promise as a means for modifying the
natural history of T2DM and warrants further study in this context. In
this report, we will review the rationale and evidence underlying this
interesting therapeutic option, and its implications for both clinical
research and the management of patients with T2DM.
http://www.ncbi.nlm.nih.gov/pubmed/22928577
Download the radio becomes important for radio lovers and language learners.
So you can imagine how much your choice has increased from
before.
Also visit my weblog ... internetradiosender
He has written a review of early insulin therapy which shows where he's coming from. As they say in the article, his position is that the remission from the intensive therapy is only temporary
'Short-term intensified insulin treatment in type 2 diabetes: long-term effects on β-cell function'
http://onlinelibrary.wiley.com/doi/10.1111/j.1463-1326.2012.01658.x/full
He says 'This apparent ‘remission’ of diabetes is likely secondary to improved β-cell function and can last for more than a year, although it is not sustained and hyperglycemia eventually will return'
Those that are more amenable to remission have : Shorter duration of T2DM, better glycemic control ,higher late-phase insulin secretion, higher BMI , higher insulin resistance, fewer chronic vascular complications, greater self-care adherence, better glycemic control .
He suggests that the remission is only partial because the beta cell dysfunction doesn't result purely from glucotoxicity but there is another component . The glucose levels (and presumably circulating FFAs which he mentions in the intro ) can be reduced by insulin but insulin may not do anything to alleviate the other component.
So what's the mystery component ? (my guess is that it varies but that's because I think T2 is probably several different conditions with differing causes but similar symptoms. )
I also think that using insulin alone doesn't address the issue of insulin resistance People with higher BMIs may initially do better with insulin because they have greater b cell mass in the first place than their thinner counterparts. ( post mortem studies suggest that they do and that people with lower BMIs have far less) However, they may also be more insulin resistant and if the pancreas is going to have to produce high levels of insulin to overcome resistance then eventually it's going to produce too little. (aging alone reduces beta cell numbers)
In the last part of the paper he says that one of the values of producing a period of remission is ' a strategy for the unbiased evaluation of the capacity of medications to preserve β-cell function in clinical trials' He's previously done a pilot where the patients had a months intensive insulin followed by sitagliptin and met or met alone. In that study B cell function declined similarly over 2 years in both arms so it doesn't appear that the drug preserved it. However, those taking the siptagliptin had better A1cs.
http://www.ncbi.nlm.nih.gov/pubmed/20920044
He's using liraglutide in conjunction with this trial. That's claimed to enhance beta cell function.and possibly to preserve beta cells. In animal studies it was found to reduce cell death . That's important because we don't seem to be able to regenerate Bcells easily. If it works better than placebo it certainly makes a different treatment path . However the downside is that the drug carries a black box warning in the US. (causes dose depend thyroid tumours in rats)
I just wanted to give you a quick heads up! Other than that, wonderful
blog!
Also visit my webpage: bmi chart male
I note the other more successful studies were earlier on. Makes a compelling case to me to consider this very early.
" state of eternal internal bliss of uninterrupted ketosis"
LOL
I hope to get around to posting on the other review paper soon ... it makes a case that IR may well be less of an issue than we think.
these statistics.
Also visit my blog post :: ralph lauren outlet online
Would you be interested in trading links or maybe guest
authoring a blog post or vice-versa? My website discusses a
lot of the same subjects as yours and I feel we could greatly benefit from each other.
If you might be interested feel free to shoot me an e-mail.
I look forward to hearing from you! Terrific blog by the way!
Here is my blog post - neo bux
With hypercortisolaemia & hyperadrenalinaemia (& probable hypomagnesaemia), I don't think so!
'Type 2 diabetes mellitus is characterized by insulin resistance and failure
of pancreatic beta-cells producing insulin. Mitochondrial dysfunction may play a
role in both processes of diabetes. Autophagy maintains cellular homeostasis
through degradation and recycling of organelles such as mitochondria. As
dysfunctional mitochondria are the main organelles removed by autophagy, we
studied the role of autophagy in diabetes using mice with beta-cell-specific
deletion of the Atg7 gene. Atg7-mutant mice showed reduction in beta-cell mass
and pancreatic insulin content. Electron microscopy showed swollen mitochondria
and other ultrastructural changes in autophagy-deficient beta-cells. Insulin
secretory function ex vivo was also impaired. As a result, Atg7-mutant mice
showed hypoinsulinemia and hyperglycemia. These results suggest that autophagy
is necessary to maintain structure, mass, and function of beta-cells. Besides
its effect on beta-cells, autophagy may affect insulin sensitivity because
mitochondrial dysfunction has been implicated in insulin resistance and
autophagy is involved in the maintenance of the organelles. Furthermore, since
aging is associated with impaired glucose tolerance, decline of autophagic activity may be involved in age-associated reduction of glucose tolerance.'
http://www.ncbi.nlm.nih.gov/pubmed/20649543
Insulin treatment probably helps because it makes beta cells take up micronutrients needed for autophagy. Magnesium, which is known to be regulated by insulin
http://www.ncbi.nlm.nih.gov/pubmed/7714114
...and manganese, which can enter cells in exchange for magnesium
http://www.ncbi.nlm.nih.gov/pubmed/3571233
It was shown earlier this year that mice with diabetes caused by a high fat diet could be cured by manganese treatment. This is a VERY big deal.
http://www.ncbi.nlm.nih.gov/pubmed/23372018
activity may be involved in age-associated reduction of glucose
tolerance.
What am I missing, Evelyn? You're feeling impatient? I wonder what Wolf was feeling when you commented, "WTF?!"
Be genuine.
Also I wasn't calling you a troll. Genuine. No snark. Look who I was responding to and about.
So let's consider your logic for a moment. Most people understand that when we say, "Paleo meals", we are referring to the diet of course, as it's a nice abbreviation for "Paleo diet meals". If I said, "Low-fat meals" or "Gluten-free meals", would you argue that fat and gluten almost certainly didn't eat meals? >.<
This is what I mean about being genuine. There is no way you misunderstood- you took the comment out of context in a deliberate attempt to make paleo seem ridiculous.
That is disingenuous.
Good to know how you roll, Evelyn. I can't imagine why Robb would take issue with your writing style. /sarcasm
IE still is the market leader and a big section of other folks
will miss your magnificent writing due to this problem.
Check out my website :: waist to hip ratio calculator
As someone who LC's to control T2D I'm in two minds over this.
On the positive side I can certainly see the physical benefits as relief from dangerous BG's would be pretty instant which is good and the increased sensitivity regained by giving your overworked pancreas some relief must also be seen as good news. It took me 8 weeks of hard work on a VLC regime to get my BG's back under control and this method would have got my levels sorted from day 1 assuming a correct insulin regime was prescribed.
On the negative side I don't see that it solves the fundamental underlying problem of ongoing safe control of T2D once that initial insulin therapy is stopped. T2D isn't just about sorting out high BG levels, just as importantly is making permanent changes to your diet and lifestyle. In my mind the key time to do that is as soon after diagnosis as possible i.e. when you are in the state of shock of being recently diagnosed. I and I suspect many T2D people who successfully control primarily by diet need something like that initial 8 week period to get their heads around the psychology of getting in a dietary control mindset for life. Insulin therapy in this case could just be an easy option and may lead to people never making the lifestyle changes required to hold the disease in check by obtaining truly safe A1C's (<6.5% in my opinion) and losing weight if they need to etc. If they don't make the required changes then pretty soon they are going to find themselves on permanent heavy insulin regimes (heavy to beat T2D insulin resistance) which will undoubtedly encourage weight gain and the associated life threatening problems that brings.
I would add that many people including myself who control by LC find that after a while their sensitivity to carbohydrates decreases (gets better) just as it does on the insulin regimes being discussed. I would argue that occurs for similar reasons in that just as the insulin regime is giving your pancreas a much needed rest a LC regime will also achieve the same thing as insulin requirements are much reduced. In my case to initially get control I dropped to a VLC 40g / day regime for the first 3 months or so. 18 months on my sensitivity has certainly doubled and maybe even trebled however I generally stick to around 75 / 80g / day simply because I know if I regularly went much higher my psychological control would undoubtedly begin to weaken.
Then you have long time low carbers who were not diabetic who now are exhibiting prediabetic FBG and/or making claims of glucose intolerance (if someone claims eating a small bowl of oatmeal will send their BG to 150-200 range, that is IGT or diabetes).
Given it's myriad roles in the human body, it would be preferable, to me anyway, to restore beta cell function and know that it is restored and insulin is being secreted and acting on adipocytes and other organs normally by consuming carbs from time to time than to "throw in the towel" on my pancreas out of misplaced notions about a hormone.
So I'd have to disagree that the EIT doesn't show long term success. Sure, not in 100%, but I would like to see studies on IGT ... I'll bet if this was done with them you'd be talking a large proportion that never proceed to diabetes. The downside to that would be?
Between EIT, GBP and the crash diet study, there seems to be an acute shock response that restores beta cell function. If weight loss on LC is rapid (as it often is) and it's not a very high fat version, perhaps then too the pancreatic fat is reduced (which appeared to be the mechanism in the crash diet study) and such a person could return to a normal diet and consider themselves cured. Have you seen this post/comparison of mine?
http://carbsanity.blogspot.com/2011/07/diabetes-crash-cures-vlcal-vs-vlcarb.html
Firstly I have no disagreement with you over a non diabetic long term LC'er who eats a potato and then is shocked by their BG response! As far as I'm aware a persons first phase insulin response in based largely on the carbohydrate content of recent meals i.e. the body "guesses" what response is needed from recent history. Consequently if you LC your recent insulin responses will be minimal thus eating a plate of starch will spike your levels, probably quite spectacularly. My attitude would be the LC'er can simply continue LC'ing if that's what they desire or they can gradually up their carbs and they should recover their first phase response pretty quickly. It's for this reason your have to consume >150g of carbs per day for more than three days to get an accurate OGTT.
Secondly on the area of reversal. I would argue that what you term hyperglycemia and T2D are two different things. I don't deny what hyperglycemia exists but that in those people where it is reversed those people are pre-diabetics and did not have full T2D. I know of several pre-diabetics (including my wife) who successfully reversed the condition so that they can consume a normal diet (whatever that is but I know what you're getting at). My wife reversed a few years ago using a classic low fat regime but I also know people who used the Newcastle diet or like myself did LC and then discovered they could "up carbs" without any detrimental effect. I don't see any reason to dispute an insulin regime such as in the study can achieve the same thing for pre-diabetics . There is patently no downside for anyone who successfully did the short term insulin regime as otherwise they risked misdiagnosis as being diabetic (subtlety different to risking proceeding to diabetes).
In true T2D though it is different. For at least 6 months and probably a lot longer I unknowingly ran with stupidly high BG's well outside the pre-diabetic range and suffered significant beta cell loss as a consequence. I agree that an initial insulin regime could have hastened both my recovery of normal BG's and hastened a moderate increase in tolerance to carbohydrate both of which my LC regime have also provided. The trouble is at the end of that insulin therapy period I don't believe I would be one of the lucky ones who found themselves reversed.
Weightloss is always important (if required) both for pre-diabetics and diabetics I'm not convinced that say the Crash diet is necessarily better than any other in reversing pre-diabetes. Effectively so long as you lose the weight you'll lose the IR. For a pre-diabetic this is what I feel fundamentally reverses the condition and for those with T2D it is that which is long term improving carb tolerance rather than any significant regeneration of beta cell mass. All regimes should restrict calories to achieve weight loss.
I do test my own carbohydrate tolerance, the last time was over the Christmas period where I doubled if not trebled my normal carbohydrate intake for about 15 days. I coped reasonably well for a couple of weeks but in the end my FBG's began to rise inexorably. By the beginning of the third week they were back to a level were I would be diagnosed T2D on a straight FBG test. If I had reversed and have been confusing myself with my own LC regime then I should have seen an initial spike in FBG's followed by a return to normal as my "repaired" first phase response came back online. It didn't but such is life ...
I would say that I've made it clear to my doctor that if for whatever reason I abandon LC I want to go straight onto insulin and miss out the only marginally effective weight gain producing meds. I have no personal fear of insulin having seen in save my sons life.
My gripe with "you-know-who" is that he poo-poos trying "A" to "Z" and just plays the trump card.
Rippln App - rippln reviews - rippln app
Stop by my blog poѕt rippln app
There is a small local farmer 3 towns away from us where I buy my pastured beef. They also sell raw dairy... and it's a small, family run farm. ~shrugs~ I suppose they are still business people though. And thank goodness for them.
As for hype, I don't believe it. I've been eating from the paleo template for almost 7 years. I'm 100 lbs leaner, I reversed the diabetes I was diagnosed with, my lipid profile is ideal, the GERD is gone as is the debilitating seasonal depression I suffered with. There is no hype here, there is simple empirical evidence. And yeah, I do sorta believe that.
~Huntress
Post a Comment
Comment Moderation is ON ... I will NOT be routinely reviewing or publishing comments at this time..