Masai Women Ate a "Low Fat" Diet
Ahh the trails that Nina Teicholz leads me down ...
In The Big Fat Surprise, Chapter 6 is entitled: How Women and Children Fare on a Low-Fat Diet. As with so many chapters in this book, this chapter begins with talk about the AHA, no RCTs, yada yada,


From BFS:
Image Summary of Post:
 |
| adapted from source gray values are calculated from original data |
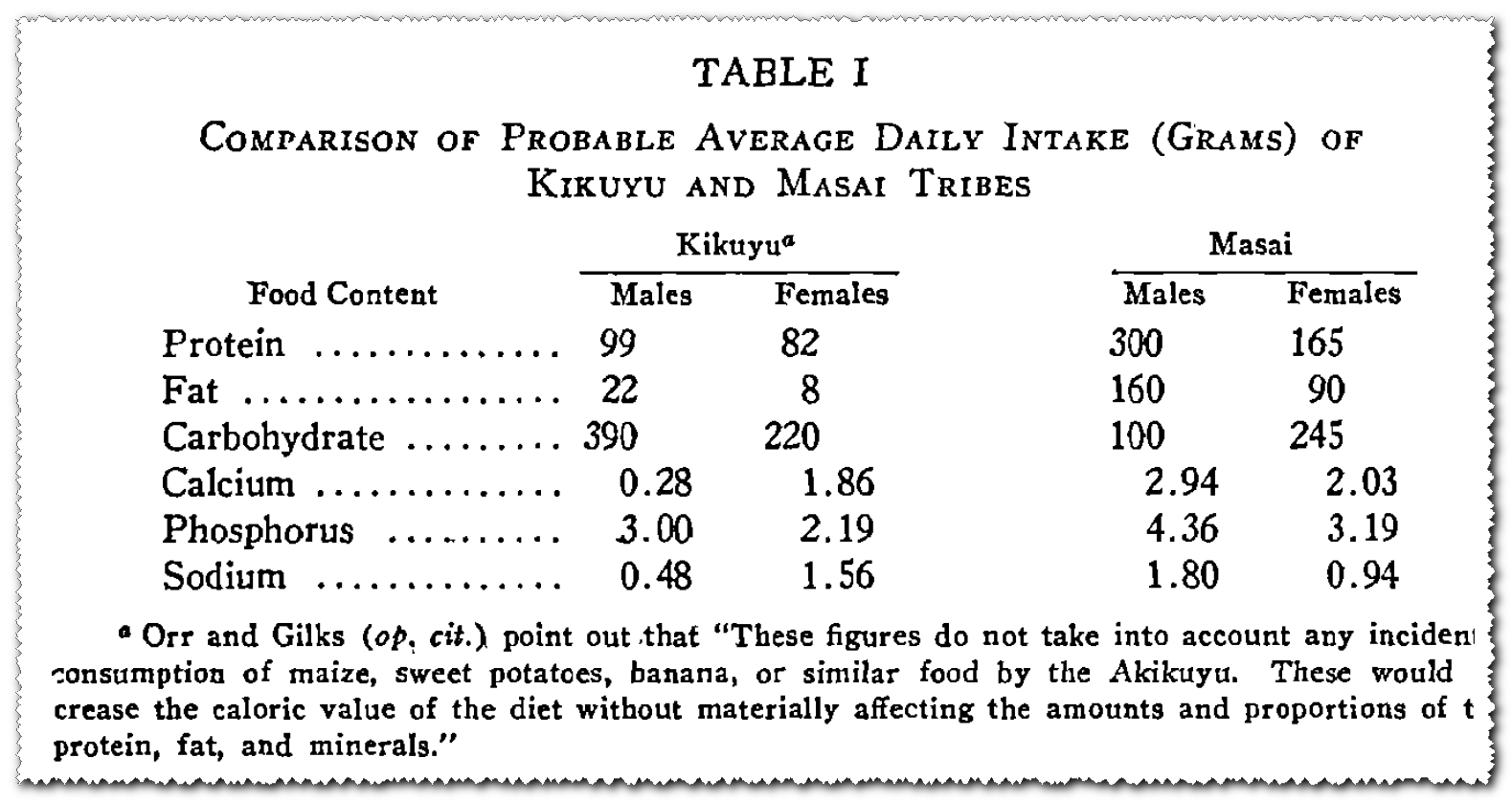
While the males of the Masai tribe consume 3040 cals/day of approximately 39%P : 47% F : 13% C, the females consume 2450 cals/day of approximately 27%P : 33% F : 40% C. Got that? Masai women, ate a "low fat" diet. This data comes from a sourced cited in The Big Fat Surprise.
The "near-vegetarian" diet of the neighboring Akikuyu tribe is more likely attributable to micronutrient deficiences, more pronounced in males due to their avoidance of "effeminite" leafy greens.
The "near-vegetarian" diet of the neighboring Akikuyu tribe is more likely attributable to micronutrient deficiences, more pronounced in males due to their avoidance of "effeminite" leafy greens.
The Women and Children Suffer Most?
In The Big Fat Surprise, Chapter 6 is entitled: How Women and Children Fare on a Low-Fat Diet. As with so many chapters in this book, this chapter begins with talk about the AHA, no RCTs, yada yada,
This idea about the cause of obesity had always been lurking in the background of the diet-heart conversation, but it did not become a formal dietary recommendation until 1970, when the AHA, ever on the forefront of ratcheting back fat, first published a guideline setting a 35 percent limit on fat as a portion of total calories.
Ooooh the horrors! Need I remind you that according to the NHANES data her newfound friend Adele Hite favors only puts fat intake at a *whopping* 36.9% for men, and 36.1% for women? Let's average that out to 36.5% and we're talking the reduction of 1.5% of total fat calories in the diet. A bit more math, using NHANES calories from here. This "ratcheting back" -- this horrific untested idea of restricting fat would have amounted to the following:
Men:
2453 cals x 0.369 = 905 cals ... 905/9 = 105 grams fat
2453 cals x 0.350 = 859 cals ... 859/9 = 95 grams fat
Reduction in fat intake = 10 grams
Women:Keep in mind, this is the PREMISE for this whole doorstop of a book! Teicholz continues on
1540 cals x 0.361 = 556 cals ... 556/9 = 62 grams fat
1540 cals x 0.350 = 539 cals ... 539/9 = 60 grams fat
Reduction in fat intake = 2 grams
In fact, the data underpinning the low-fat diet amounted to only a couple of tiny studies, one from Hungary and one from Britain, in which fat was severely reduced to an unrealistic 1.5 ounces a day to see if such a diet could reduce heart disease. And these two studies had contradictory results. Trials aimed at testing the 35 percent fat limit that was already being recommended had simply not been performed.
Firstly, 1.5 ounces in terms of grams gives a number folks are more familiar with for macronutrients: 1.5 oz = 42 grams. This is hardly unrealistic, for example the Thai diet I discussed here
Secondly, considering the notorious lack of compliance in actual clinical trials, I'd say that the grand experiment beginning with 35% fat had been long underway. Lastly, all is 35% is the cut-off for the dangerous low fat diet now? From Teicholz's own rendition of the 1950 (sic) Yerushalmy & Hilleboe Data --
The women and children, remember?
Oh yeah, the chapter is about how the weak among us fare. In adopting a diet advised for middle aged men, we have suffered so. As occurs throughout the book, the chapter titles in BFS fail to summarize the content or focus of the chapter. The chapter opens with discussions of Snackwells and mention of the food industry, Honey Nut Cheerios gratuitous Usher video embed), and Quaker Oats ... AHA, "Heart Healthy" and "prudent".
Did you know?
For instance, the major American yogurt manufacturers to this day sell only low- or nonfat yogurts. (In 2013, the only full- fat yogurts on the national market came from Greece.)
This is perhaps technically true, by inserting "national market", but full fat plain yogurt has been sold all along. This should be celebrated by the fructophobes, because it's the flavored yogurts where the fat was cut. But my folks have been eating Stonyfield Farms yogurt for years now (and others before that). I'm pretty sure most Greek yogurts that are all the rage, don't actually come from Greece (Oikos is a Dannon brand), but I digress ... and if my facts are wrong, please feel free to set me straight in comments ;-)
So we continue on in the chapter ... next section is about Ornish and his "near-vegetarian" diet. How many Americans even come close to following Ornish? It was Atkins that was all the rage a little over a decade ago, but unlike Atkins, Ornish was an internist with no research training. What's that? Oh yeah, sorry. Just reciting from BFS, I know Atkins had no research training either and is arguably far more famous than Ornish. The Americans eating near-vegetarian diet nonsense is just that. I don't think I even know anyone who has done the Ornish diet in real life. Why is Teicholz going on about the Ornish diet? Thirty-to thirty-five percent fat ... right? The Ornish fluff is distractionary here. The Dietary Guidelines have never been anything approximating Ornish, and Americans have failed to reduce fat to the 30% suggested in the original 1977 report (which wouldn't make it into the actual Guidelines until 1990).
The Masai (... and the Akikuyu)
From BFS:
Since we now live in a time when the vegetarian (or near-vegetarian) diet is so heavily favored by health authorities as well as the popular press, these researcher findings are probably a surprise, but they would not have been to nutrition experts in the 1920s. Remember those Masai warriors in Kenya who ate little other than milk, blood , and meat? Decades before George Mann arrived in Kenya, the British government commissioned scientists in 1926 to compare the Masai to a neighboring tribe, the Akikuyu. They had lived side by side for many generations, in “very similar” conditions, according to the researchers. However, whereas the Masai ate mainly animal foods, the Akikuyu subsisted on a near-vegetarian diet that was very low in fat, with the “great bulk ” of their food consisting of “cereals, tubers, plantains, legumes, and green leaves.”
Investigators spent several years in detailed examination of 6,349 Akikuyu and 1,546 Masai adults, and in the end, found that the health of the two groups differed dramatically, though not in ways one might expect. The vegetarian Akikuyu men were found to be far more likely to suffer from bone deformities, dental caries, anemia, lung disease, ulcers, and blood disorders; the Masai were more likely to contract rheumatoid arthritis. The Masai men were on average 5 inches taller than the Akikuyu and 23 pounds heavier, and much of that extra weight was apparently muscle, since the Masai had narrower waists and broader shoulders and possessed far more muscular strength than the Akikuyu, who were generally less fit and had little capacity for manual labor. VIII
Why is the theme song from Two and a Half Men running through my head? What do the men have to do with this? This is supposed to be a chapter about how women fare on low fat diets. As it turns out, with so many of Teicholz's sources, the original citation could not be located (Orr and Gilks, 1931). I was, however, able to find an accounting of this in Biochemical Studies of Nutritional Problems, by Drummond, which as luck would have it, Google has the relevant pages freely available online! It is true that the Akikuyu suffered malnutrition on their almost vegetarian diet. But as is usually the case, the complete picture is not nearly as simple as Masai eat meat = healthy.
In Chapter 1, Teicholz introduces us to the Masai as follows:
Mann had heard that the Masai men ate nothing but meat, blood, and milk— a diet, like the Inuits’, comprised of almost entirely animal fat— and that they considered fruits and vegetables fit to be eaten only by cows.
Again ... this is the men. So not only is this an isolated pocket of humanity but we're talking the "warrior" class of men and thus ignoring the diets of women of all ages, and the children and older adults of both genders. I guess these might be the cows? I'll use the entire table later, but this is Table I crunched down a bit to focus on Masai only, and with calculated values added in gray.
|
THE MASAI WOMEN ATE LESS FAT THAN AMERICAN WOMEN IN 1970 |
Paging Mark Sisson! These women must have been insidiously fat!! Actually that looks a lot like the LoBAG-40 diet ;-) By percentage it is not nearly as high as many cultures, but this is due to the high protein content of their diet.
So now, let's put the Akikuyu back into the mix:
And then, there is this from Drummond, following a discussion of the high rate of health issues in Akikuyu children:
 |
| Akikuyu males: 2154 cals/day of approximately 18%P : 9% F : 72% C Akikuyu females: 1280 cals/day of approximately 26%P : 6% F : 69% C |
I would note that the Akikuyu males consumed some 300 cals/day less than Masai women! If Teicholz (and others) are using this source for Orr and Gilks, they probably seized on the following passage:
A large proportion of their ill health is believed on good grounds to be caused by faulty nutrition, for their diet is poor in fat, heavily overweighted with carbohydrate, and inadequate as regards calcium and at least two of the vitamins (Table I).
Lots of image repeats in this post, but compared to the Thai data I copied below, the Akikuyu men were eating roughly the average grams of fat per day as the Thai population through the mid 1970s.
The Akiyuku women are in true "danger" territory with fat intake if some are to be believed. They are also consuming just over half of their Masai counterparts in total calories. Looking at the protein, one might think the Akikuyu are deficient there as well, but the Thai (and they are not alone) consumed roughly half as much. As to "overweighted with carbohydrate", there are enough examples of healthy cultures consuming this amount to healthy outcomes.
To repeat from BFS:
The vegetarian Akikuyu men were found to be far more likely to suffer from bone deformities, dental caries, anemia, lung disease, ulcers, and blood disorders; the Masai were more likely to contract rheumatoid arthritis. The Masai men were on average 5 inches taller than the Akikuyu and 23 pounds heavier, and much of that extra weight was apparently muscle, since the Masai had narrower waists and broader shoulders and possessed far more muscular strength than the Akikuyu, who were generally less fit and had little capacity for manual labor.VIII
From the a footnote:
VIII. Muscular strength of the hands was assessed with a dynamometer, which measures mechanical force . With this test, the Masai were found to be 50 percent stronger than the Akikuyu. Another sign of physical weakness among the Akikuyu men was that 65 percent were “immediately rejected on medical grounds” when turning up for army reserve service in 1917. The women of the two tribes, by contrast, had more similar diets and did not have such dramatic differences in health (Orr and Gilks 1931, 9 and 17 “immediately rejected”).
What's that? The WOMEN ? Why is that piece of information relegated to a footnote in a chapter entitled How Women and Children Fare on a Low-Fat Diet ??? Why is there no mention of the differences between the Akikuyu men and women?
Here is the quote from Drummond
The Masai are a pastoral tribe of good physique who live almost exclusively on meat, milk, and fresh blood. Their neighbors, the Akikuyu, are agriculturalists, and although they maintain herds of goat: these are regarded as a form of currency and are rarely used to provide meat or milk. The diet of the men is almost entirely composed of cereals and potatoes, but, it being considered effeminate to eat green vegetables, these enter the diet only of the womenfolk.
As an aside, Mann describes their diet as much more milk heavy, as the cows are prized for their milk and meat would be more rarely consumed. One would expect the meat they did eat to be quite lean, though not as lean as wild buffalo. The above paragraph is followed by:
The Akikuyu men are weedy and unhealthy; Orr and Gilks quote Tate as stating that of 16,754 men of one district of the Reserve who were called up during 1917 for enrolment in the Carrier Corps no less than 12,767 were rejected on medical grounds. A large proportion of their ill health is believed on good grounds to be caused by faulty nutrition is believed on good grounds to be caused by faulty nutrition, for their diet is poor in fat, heavily overweighted with carbohydrate, and inadequate as regards calcium and at least two of the vitamins (Table I).
I grayed the repeat from earlier. Taken together with intakes of other human cultures, one must then compare within the culture. The Akikuyu women ate almost as much protein as the men, and a rather high percentage of their diet by Western standards (26% vs. 15%). They ate an almost no fat diet! By percent they are at 6%, but in absolute amount it is even more "alarming". Eight (8) grams is a scant gram over one-half of a tablespoon!! So, if the low fat content of the male diets is the cause of their ill health, one would expect the women to fare even worse consuming less than a third as much.
It is interesting to note that the incidence of defects which can be ascribed to a large extent to one form or other of malnutrition is lower in the Kikuyu girls than in the boys. This is doubtless related to the fact that the women and girls of the tribe consume a certain amount of green foods which, as has been remarked, are usually ignored by the males.
That's funny, Teicholz describes the diet of the Akikuyu men as containing "green leaves". Just another "mistake" eh? This is wrong. The women ate the green leaves. Not only that, consumption of same is credited with why they tend to be healthier than their male counterparts, and fare more similarly ot the Masai women. Look at the nutrients. The Akikuyu women may still be micronutrient deficient or on the verge of it, but not nearly to the degree as the men. Their numbers for the minerals listed vie with those of the Masai even if a bit lower. If they ate more, their diets would be contain higher absolute amounts of micronutrients than those of the Masai men or women!! Lastly, the Akikuyu women consume 2.5X the carbohydrate of the men. If excessive carbs were associated with poor health, they should be less healthy.
The Rest of the Chapter
So having thrown in the Masai & Akikuyu anecdote about the men, Teicholz moved on to address the children. There's lots of talk of infants, and the wisdom of PUFA in baby formula, etc. This is further to distract. Human breast milk should be as nutritionally matched as possible if formula replaces it, and whatever research, marketing, etc. is involved there, this really is a separate issue from adult nutrition. So we can turn to the toddlers on up in age, and there may be some point. Dairy fat -- cream and butter -- have long been helpful in preventing malnutrition in children. I actually agree with the critics of low dairy fat recommendations for children. Full fat whole milk would be preferable to low fat chocolate milk any day in my book.
However, in this country, even "junk" food is enriched and we are way past the days of the 1800s-through-early-1900s where true childhood malnutrition was an issue. Perhaps a separate issue for a future post. But if you stand back and look at humanity as a whole, there are simply too many cultures -- the Japanese from Y&H data at 8% fat, the Pima at around 10% fat, the Thai as above, even the Akikuyu women, and countless billions upon billions of humans around the globe -- thriving on diets that are far lower in fat to even consider 30% a level that might approach dangerous. Teicholz is simply way off base here, as is pretty much anyone claiming the US is suffering from any sort of fat deficiency or carbohydrate addiction.
Teicholz then moves on to discuss some rat studies where vegetarian rats fared more poorly than those fed some animal food. Rats?? OK. Let's look at how they fare on the high fat diet .... Please. Ignore all low fat cultures of humans enjoying good health, but rats? OK. But interestingly enough, green leafy veggies. Paging Zoe Harcombe!
Teicholz moves on to the wisdom of prescribing one diet for all members of the family. But the thing is, her own examples in the book -- including the hunter-gather Plains Indians -- would include women and children who DO consume less fat and protein and more carbohydrate vs. their male counterparts. Thus if anyone should complain, I suppose, it should be the men for being told to eat like a woman!
So with that set up, Teicholz goes on to discuss a number of trials on children, and women and cholesterol -- which is different from total fat as well. I simply do not have time to discuss these in detail in this post. Perhaps at some later date ... I'm only 1 year into researching Teicholz's sources ;-)
She ends the chapter on women and children with this set up for the Mediterranean diet:
Teicholz then moves on to discuss some rat studies where vegetarian rats fared more poorly than those fed some animal food. Rats?? OK. Let's look at how they fare on the high fat diet .... Please. Ignore all low fat cultures of humans enjoying good health, but rats? OK. But interestingly enough, green leafy veggies. Paging Zoe Harcombe!
Teicholz moves on to the wisdom of prescribing one diet for all members of the family. But the thing is, her own examples in the book -- including the hunter-gather Plains Indians -- would include women and children who DO consume less fat and protein and more carbohydrate vs. their male counterparts. Thus if anyone should complain, I suppose, it should be the men for being told to eat like a woman!
So with that set up, Teicholz goes on to discuss a number of trials on children, and women and cholesterol -- which is different from total fat as well. I simply do not have time to discuss these in detail in this post. Perhaps at some later date ... I'm only 1 year into researching Teicholz's sources ;-)
Big Olive to the Rescue!
She ends the chapter on women and children with this set up for the Mediterranean diet:
Of course many of us who’ve been paying attention to the science have been welcoming fat back into our diets for some time already. We’ve given up spraying with Pam, stopped poaching, and started using salad dressings again. And if there’s a silver lining to those low-fat years, it’s this: we learned that fat is the soul of flavor. Food is tasteless and cooking nearly impossible without fat. Fat is essential in the kitchen to produce crispness and to thicken sauces. It is crucial in conveying flavors. It makes baked goods flaky, moist, and light. And fat has many other, essential functions in cooking and baking. To satisfy all these compelling needs, nutrition experts coming out of the low- to non-fat 1980s and looking for a solution found one apparently perfect candidate: olive oil. And that is one of the reasons why, in the early 1990s, the “Mediterranean Diet” entered the picture.Leaving aside how laughable it is that Teicholz uses the collective "us" to describe herself as paying attention to science ... cough ... gag ... cough ... would olive oil be the same fat that includes the healthy MUFA we can find in pork? And I also can't help but laugh about the cooking lesson. Low carbers are forced to learn the touchy practice of using egg yolks as a thickener and/or resorting to using things like guar gum to thicken anything. Baked goods? Thanks for pointing out that many of these "carbs" contain fat. If over a quarter cup of fat isn't enough for you to cook 2000 calories worth of tasty food, perhaps it's your technique that's the problem.
Comments
"Since we now live in a time when the vegetarian (or near-vegetarian) diet is so heavily favored by health authorities as well as the popular press"
Does Nina offer ANY proof for this inane statement??
I generally regard the Ornish diet as extreme as the very low-carb diets, but the thing that jumped out the most at me from reading the Berkeley piece was how the author described the diet. They went over the evidence in favor as well as possible negative consequences such as higher triglycerides, and they even pointed out that it is difficult to adhere to. Yet the didn't lay out any oversimple, alternate hypotheses physiological mechanisms, pedantic take home lessons about biochemistry, rail against dietary guidelines, nor attempt to revise the history, prehistory, and evolutionary history of the entire human race to suggest all the longest-lived, healthiest individuals ever ate was the Ornish diet. All rookie mistakes, I think.
http://circ.ahajournals.org/content/98/9/935.full
Results from a few clinical trials suggest that very low fat diets are associated with reduced risk of cardiovascular disease,but numerous unanswered questions remain that make population-wide recommendations of such diets premature... Responses to any dietary intervention designed to alter blood lipid levels or body weight vary among individuals. Data are still lacking from randomized clinical trials in which representative population samples with adequate power were used to test whether there is substantial additional benefit to be derived from very low fat diets. Because very low fat diets represent a radical departure from the current prudent dietary guidelines, such diets must be proved both advantageous and safe before national recommendations can be issued.
Odd, it's really out of character for the AHA subject Americans to a vast, uncontrolled diet experiment with potentially disastrous consequences. Oh well.
Here's another statement I like:
Because weight loss frequently accompanies the initial adoption of a very low fat diet and independently affects blood lipid levels and cardiovascular risk, assessing the effect of the very low fat diet alone is difficult.
You could almost replace the words "very low fat" with "very low carb."
> Lastly, all is 35% is the cut-off for the dangerous low fat diet now?
#1 should read: Lastly, is 35% now the cut-off for the dangerous low fat diet?
#2 ended up being a mix between "fairer sex" and "weak among us" ... it needs quotes on the weak, and just get rid of fair. :)
I would hypothesize that one reason the low-fat vegan approach works so well is because it automatically reduces linoleic acid intake to a safe level. In contrast, low-fat gorilla chow caused heart disease because the linoleic acid content exceeded 3% of calories and the sugar content was too high. Even adding vitamin E to the chow did not furnish protection from excessive linoleic acid intake. Consequently, gorillas in American zoos got heart disease on a low-fat vegan diet. "Identified as a leading cause of death in great apes living in zoological settings, cardiovascular disease (CVD) requires advanced understanding of diagnosing, treating and monitoring affected individuals, as well as adapting techniques already in use for treatment of heart disease in humans and domestic animals." Google - gorilla biscuits Cleveland Zoo
sad stuff happens when one ignores most media for a long time
Terry Pratchett has died.
I'll miss him.
SO - the question is how much of the benefits of the Ornish Program come from the diet and how much come from the non-diet elements??
https://disqus.com/by/disqus_FCYY9GDhJe/
Foreword
by Sir Heneage Ogilvie
From Eat Fat & Grow Slim (1958)
"There are three kinds of food: fats, proteins and carbohydrates. All of these provide calories; the fats 9.3 calories per gramme, the proteins and the carbohydrates 4.1 each. But the carbohydrates provide calories and nothing else.
They have none of the essential elements to build up or to repair the tissues of the body. A man given carbohydrates alone, however liberally, would starve to death on calories, While he was dying he would break down his own proteins to provide materials for the repair of his key organs. He would use what calories were needed to provide energy, and he would lay down the carbohydrate surplus to his caloric requirements as fat.
Proteins are the essential food of the body. They provide not merely carbon, nitrogen, sulphur, phosphorus, sodium, potassium, calcium and iron, chlorine and iodine, but those trace elements such as boron, manganese, zinc, copper, and cobalt that are essential to life. They provide many prefabricated molecules that the body is unable to build up from simple elements.
Fat is the caloric reserve material of nature. The whale stores fat in his subcutaneous layers against the rigours of life at the Pole, the camel stores it in his hump against hard times in the desert, the African sheep stores it in his tail and his buttocks against the day when even the parched grass shall have withered away. But fats are more than stores of reserve caloric material. They are heat insulators, they are fillers of dead spaces, and they are facilitators of movement in rigid compartments such as the orbit, the pelvis, and the capsules of joints. They are also essential building materials. Animal fats contain three groups of substances: the neutral fats which are chiefly energy providers, the lipids containing phosphorus that enter into most tissues and bulk largely in the brain and the central nervous system, and the sterols that are the basis of most hormones.
The body must have proteins and animal fats. It has no need for carbohydrates, and, given the two essential foodstuffs, it can get all the calories it needs from them.
The expert on nutrition is not the nutrition expert, but the man who has studied nutrition by the ultimate method of research, the struggle for survival. The Eskimo, living on the ice floes of the North Pole, the Red Indian travelling hard and far over wild lands in hunting or war, the trapper in the Canadian forests, the game hunters in Africa-these men must find food that gives the greatest nutritive value in the smallest bulk. If they cannot find such a diet, their journeys will be limited both in time and in distance, and they will fail in their task All these men have found that a diet of meat and animal fat alone, with no carbohydrates, with no fruit or vegetables, with no vitamins other than those they get in meat, not merely provides them with all the energy they need, but keeps them in perfect health for months at a time. Seal meat and blubber for the Eskimo, pemmican for the Indian and the trapper, biltong for the hunter, have proved to be the perfect diet both in quality and in bulk."
With its $40 million, too bad NuSI doesn't have the guts to do a similar long term trial with LCHF.
"I have lost 48 pounds. My blood work has gone from total cholesterol of 208, LDL of 93, HDL of 41, and triglycerides of 368 last June to most recent results of total cholesterol of 89, LDL of 19, HDL of 53, and triglycerides of 83. That transformation is nothing short of amazing."
Almost entirely animal fat. Does Teicholz think the Inuit ate hardly any meat, just fat? This would be interesting, because that's approximately what Mike Eades thinks, and there's a debate on his blog about it. His idea is that the traditional Inuit diet was ketogenic, and that ketosis is the natural human state. His opponents are telling him the evidence says the Inuit were not in ketosis and ate enormous quantities of meat. I wonder what Taubes and Attia think about this. Do they think the Inuit were in ketosis too? Did Teicholz get it from Taubes? I am also wondering what people like DiNicolantonio and Harcombe think. And the folks at Open Heart. Do they all believe what Mike Eades believes?
Anyway, do you know what Taubes and Attia think about it? I get the feeling that Eades has some serious backup.
'Proteins are the essential food of the body. They provide not merely
carbon, nitrogen, sulphur, phosphorus, sodium, potassium, calcium and
iron, chlorine and iodine, but those trace elements such as boron,
manganese, zinc, copper, and cobalt that are essential to life.'
Proteins provide all these elements do they, and carbohydrates do not. Hmmmm.
The Eskimos survived on their diet by necessity.
http://www.ncbi.nlm.nih.gov/pubmed/17928161
"....Low copper and cytochrome oxidase in Alzheimer brain can be attributed to low copper intakes or higher than average nutritional requirements. Experiments with animals deficient in copper involving amyloid, ceruloplasmin, copper transport, cytochrome oxidase, myelination, organ analysis and oxidative defense are consonant. Decreased cognition and increased tau in cerebrospinal fluid in Alzheimer's disease also are associated with low copper status. A high requirement for copper may explain early onset of Alzheimer's disease in Down's syndrome. Copper deficiency is a plausible cause of Alzheimer's disease. ...."
and manganese deficiency
http://www.ncbi.nlm.nih.gov/pubmed/22892312
"Using cultured cortical neurons, we show that the blockade of protein phosphatase 2A (PP2A) ... inhibited basal autophagy and autophagy induced in several experimental settings....These data are important to human neurodegenerative diseases, especially Alzheimer's disease, because they provide links for the first time between the pathological features of Alzheimer's disease: PP2A downregulation, autophagy disruption, and protein aggregation." [PP2A is a manganese enzyme]
.....but I couldn't find anyone who would forward it to him.
http://www.jfponline.com/fileadmin/qhi/jfp/pdfs/6307/JFP_06307_Article1.pdf
Its results suggest (at least to me) that the diet effect was substantial and imperative. Esselstyn's diet is even more extreme than Ornish's, but the sole intervention is diet, no meditation or exercise is required (though both are suggested).
If I had CVD, I'd give Esselstyn's prescription a try because as a prescription to counter an existing condition, I think he's demonstrated efficacy. As a means of prevention though, that extreme of a diet holds little appeal to me.
Also - no info was provided about the diet with regard to calories, macro nutrient ratios, etc. Would have been useful as well.
By the way, I am not a LCHF enthusiast.
Abstract
Disturbed copper (Cu) homeostasis may be associated with the pathological processes in Alzheimer's disease (AD). In the present report, we evaluated the efficacy of oral Cu supplementation in the treatment of AD in a prospective, randomized, double-blind, placebo-controlled phase 2 clinical trial in patients with mild AD for 12 months. Sixty-eight subjects were randomized. The treatment was well-tolerated. There were however no significant differences in primary outcome measures (Alzheimer's Disease Assessment Scale, Cognitive subscale, Mini Mental Status Examination) between the verum [Cu-(II)-orotate-dihydrate; 8 mg Cu daily] and the placebo group. Despite a number of findings supporting the hypothesis of environmental Cu modulating AD, our results demonstrate that oral Cu intake has neither a detrimental nor a promoting effect on the progression of AD.
http://www.ncbi.nlm.nih.gov/pubmed/18587525
I agree, more data would be better.
Not everyone thinks clogged arteries are big deal. For instance Nina Teicholz in a recent debate with John Mackey (of Whole Foods) stated that cholesterol build up in blood vessels isn't a big deal unless the clots break off. Me? I think unclogged beats clogged all day, every day.
All that dietary fat has crossed his BBB, that's where the backup is.
Linoleic acid is already on the long list of potentially toxic food components I've seen espoused by bloggers. Everything is toxic at some dose or in some context. As Kevin points out on his blog nutrients don't act in isolation, and arguing over fatty acid is silly http://nutrevolve.blogspot.com/2014/11/war-of-worlds-butter-vs-oil.html I'm generally responsive to the notion that it was a mistake to demonize individual nutrients like saturated fat, fat, etc. This compromised people's confidence in the credibility of nutritional science. What gets me is how people can then take a 180 degree turn and start blaming health problems on things like carbs, gluten, fructose, linoleic acid, etc.
Elsewhere on this blog I've explained to Evelyn why I feel linoleic acid is not simply "a dietary bogeyman" as you put it. You folks who follow this blog are pretty sharp. If I'm mistaken, then some more eyes on the research may be needed to set me straight.
Kevin is correct. Nutrients do not act in isolation. However, there is evidence from Joseph Hibbeln's research of a dramatic difference in the effects of 1% and 8% linoleic acid independent of the fat/carb mix. Google - Joseph Hibbeln Omega-6
Excerpts:
"When we deleted that one single molecule, the Omega 6 fatty acid, we were able to obliterate the ability of a 60% high fat diet to induce obesity in the mice...And we did it also in diets that were 35% of calories from fat, and also diets that were 12% of calories from fat. We were able to induce obesity in low fat diets, in the mice, by changing the bioactive properties of the fat, not just that it was high fat and more calories."
http://wholehealthsource.blogspot.ca/2011/08/seed-oils-and-body-fatness-problematic.html
thanks for the tip, I'll have to fin those Hibbeln papers
I contest very little of what Dr. Willett says. However, his advice to lower LDL-C by swapping linoleic acid for saturated fat would make sense only if lowering LDL-C were to prove beneficial. This has yet to be done in any meaningful way by dietary means related to saturated fat and linoleic acid intake. If such an approach were truly effective, preventing heart disease would be a snap. And captive gorillas would not have developed heart on gorilla biscuit rations containing 6.5% soybean oil as the only fat ingredient. Interestingly, on Page 94 of a January 2012 dissertation entitled ADIPOSITY IN ZOO GORILLAS (GORILLA GORILLA GORILLA): THE EFFECTS
OF DIET AND BEHAVIOR by Elena Hoellein Less one reads, "Biscuits may be a healthy diet item as the only source of fiber, but the high levels of sugar, starch and saturated fat they contain could have deleterious health effects" (Note - soybean oil contains about 55% linoleic acid and about 16% saturated fats). Also of interest is the fact that the animals lost weight despite increased caloric intake. Page 119: "Institutions need to be prepared for weight loss even if kilocalories are doubled."
A couple days ago I listened to a debate between Nina Teicholz and John Mackey. I found it interesting that Mackey asserted that "gorillas are a lot like humans." If he's correct, than even low levels of linoleic acid intake along with what used to be considered benign levels of sugar intake for gorillas is deadly. Google - gorilla biscuits Cleveland Zoo
http://www.ncbi.nlm.nih.gov/pubmed/24081493
http://www.ncbi.nlm.nih.gov/pubmed/22334255
A few days ago I found an article on corn oil and appetite reinforcement that may be related to Hibbeln's research. Google - corn oil effective reinforcer
Now, a new study that makes use of powerful databases of genetic information has found that raising HDL levels may not make any difference to heart disease risk. People who inherit genes that give them naturally higher HDL levels throughout life have no less heart disease than those who inherit genes that give them slightly lower levels. If HDL were protective, those with genes causing higher levels should have had less heart disease.
http://www.thelancet.com/journals/lancet/article/PIIS0140-6736%2812%2960312-2/fulltext
Plasma HDL cholesterol and risk of myocardial infarction: a mendelian randomisation study
Interpretation
Some genetic mechanisms that raise plasma HDL cholesterol do not seem to lower risk of myocardial infarction. These data challenge the concept that raising of plasma HDL cholesterol will uniformly translate into reductions in risk of myocardial infarction.
Discussion
For a biomarker directly involved in disease pathogenesis, we expect a genetic variant that modulates the biomarker to likewise confer risk of disease. We tested this hypothesis for two plasma biomarkers: LDL and HDL cholesterol. SNPs affecting LDL cholesterol were consistently related to risk of myocardial infarction. However, we unexpectedly found that LIPG Asn396Ser, a genetic variant that specifically and substantially increases plasma HDL cholesterol, did not reduce risk of myocardial infarction. A genetic score combining 14 variants exclusively related to HDL cholesterol also showed no association with risk of myocardial infarction
I'm not really concerned with this entire issue because I think that cholesterol is not a problem except for those who have genetic abnormalities. For the average person, the body adjusts cholesterol for the individual.
I was just surprised at the idea that high HDL is not protective, since that's not only what I've been told by doctors but what I've read as well.
Nobody could induce CVD in an animal with sugar-feeding alone the way they could with saturated fat or cholesterol (or for faster CVD yet, the two together), plus, before the Age of Obesity, there were countries with high sugar intake but low rates of CVD (Cuba, Venezuela).
Now here we are decades later and after a careful review of all the science, the World Health Organization says sugar is really bad for…wait for it… your teeth.
Anything else?
http://instantrimshot.com/audio/crickets.mp3
The latest WHO report is notable for what it doesn’t say about sugar. It doesn’t say sugar is addictive, toxic, uniquely fattening, or that it gives you fatty liver, heart disease or diabetes. That’s because these are all just myths peddled by attention-seeking, non-nutritionists to boost their celebrity, sell books and make money.
Too much sugar is bad for your teeth. And sugar contains calories, which cause weight gain when consumed in excess of the body’s needs.
It’s not rocket science; it’s nutrition science.
- See more at:
Modern Diet Myth No. 6: Sugar is really, really bad for you
See more at: http://scepticalnutritionist.com.au/?p=1844#sthash.H2op0Xn7.dpuf
The history of sugar bashing doesn't even begin until around 2003-2004. Take a look at the article dates in the references for this 2009 article. http://www.ncbi.nlm.nih.gov/pmc/articles/PMC3210834/ The AHA never issued a strongly worded warning regarding added sugars until 2009. http://circ.ahajournals.org/content/120/11/1011.full
The argument that sugar alone can't be causing the obesity epidemic is based on the fact that, on average, slender people consume more sugar than fat people. True. But slender people have a different metabolic response to high sugar intake from fat people as noted in this research. "It was necessary to raise the daily carbohydrate intake to 85-90% of the total daily caloric intake in order to induce hyperglyceridemia in normolipemic subjects." http://ajcn.nutrition.org/content/20/2/116.abstract
The idea that high HDL is not 'protective' actually focuses on why it's always 'associated' with good heart health. What seems to be the area of further study are the reasons for LOW HDL--which IS associated with cardiac risk. The report mentioned so many other poor lifestyle habits that seem to be connected to those with low HDL and may be the actual cause of cardiac issues--perhaps in combination rather than a single factor.
But there is no indication at all that high HDL is any type of 'problem' for those (like myself) for whom this is a natural occurrence. What they are now questioning are efforts to raise HDL alone because the assumption that the low HDL was the only negative factor is now questioned. That makes sense, but there's no indication that my high HDL is at all a risk factor. In terms of 'heart health,' my doctors look at a variety of issues, my lipids are just one of many things that are checked.
Add a pound of full-fat cheese and garnish with a half dozen avocados and it's still 100% vegetarian.
Throw in Costco-sized containers of coconut oil, olive oil, almonds and macadamia nuts, and it's still 100% vegetarian.
Chase it down with a gallon of "Primal Fuel" mixed with your "Bulletproof coffee" and it's still 100% vegetarian.
In truth, nearly everyone eats a "near-vegetarian" diet, even the Paleo HFLC types.
http://freetheanimal.com/2014/10/damned-inuit-diet.html
Davos 2015 - Let Food Be Thy Medicine
How can our daily diet and dietary habits become a cornerstone of health?
Dimensions to be addressed:
- Role of nutrition in tackling disease
- Impact of traditional culinary systems
- Need for global dietary guidelines
• David B. Agus, Professor of Medicine and Engineering, USC Center for Applied Molecular Medicine, USA; Global Agenda Council on the Future of the Health Sector
• Simin Nikbin Meydani, Director, Jean Mayer USDA Human Nutrition Research Center on Aging, Tufts University, USA
• Dean Ornish, Founder, President and Director, Preventive Medicine Research Institute, USA
• Joan Roca, Chef, El Celler de Can Roca, Spain
Moderated by
• Mariette DiChristina, Editor-in-Chief, Scientific American, USA; Meta-Council on Emerging Technologies
http://www.ncbi.nlm.nih.gov/pmc/articles/PMC3504986/
Sure LDL-P is thought to be a greater risk factor than LDL-C, but what I would want to know is if there's yet standard LDL-P test that can be used in a normal, evidence-based clinical practice? Also, given that LDL-C targets have been abandoned is there any outcomes research for either assessing risk from or targeting LDL-P? I've also found advocates of ketogenic and LCHF diets to be very biased, yet they do often anecdotally show desirable lipid profiles. I would love to see an unbiased review the effects of ketosis on lipids.
That has nothing to do with my naturally high level--and it gives no reason for my doctors NOT to believe that my numbers are a good thing--given my other lab results which they are observing at the same time.
Moreover, there are MANY other studies that show the importance of high HDL, so this single study is more speculative than definitive--which is common with 'studies' that are mainly reported in the press.
Again, it's time to end this discussion.
However ... One thing that is bugging me is the Vitamin E thing you mentioned. I looked up sources of linoleic acid, and lo and behold many are on lists for good sources of VitE. Am I missing something?
Also, since I'm on the African tribe kick, I remembered the Kalahari bushmen consuming mongongo nuts that I mentioned here: http://carbsanity.blogspot.com/2015/01/h-g-food-procurement-strategies.html
So here is what I found about mongongo nut nutrition: http://www.naturalhub.com/natural_food_guide_nuts_uncommon_ricinodendron_rautanenii.htm
>>>"Nutritional value of the kernel Their nutritional content is outstanding. The kernel is 57% by weight fat. Of this, about 43% are polyunsaturated fats (almost entirely linoleic acid), about 17% saturated fats (palmitic and stearic), and about 18% monounsaturated (oleic). Add the sugars in the fleshy part, and, by one estimate, an adult man would meet 71% of his daily energy requirement by eating 100 fruits (kernels and flesh). Indigenous people have been reported as eating around 100-300 fruit a day in parts of Namibia.
The kernel has 26 grams of protein per 100grams, an amount similar to peanuts and other protein rich legumes.
The kernel has, per 100 grams, approximately 193 mg of calcium, 527 mg magnesium, 3.7 mg iron, 2.8 mg copper, 4 mg zinc, 0.3 mg thiamine, 0.2 mg riboflavin, 0.3 mg nicotinic acid, no vitamin C (the flesh has about 15 mg), and a stunning 565mg of vitamin e (almost entirely as y-tocopherol).[1] Due to the very high y-tocopherol content, the oil is very stable, and doesn't oxidise into 'rancidity' for a very long time, in spite of the African heat. "<<<
dietary LA was associated with a 15% lower risk of CHD events and a 21%
lower risk of CHD deaths. A 5% of energy increment in LA intake replacing energy from saturated
fat intake was associated with a 9% lower risk of CHD events and a 13% lower risk of CHD deaths." http://www.ncbi.nlm.nih.gov/pubmed/25161045
In contrast, Joseph Hibbeln says, "... when that dietary advice was interpreted to replace saturates with
Omega 6, linoleic acid, that advice looks to be very harmful." http://www.meandmydiabetes.com/2013/03/10/vegetable-oil-associated-with-more-heart-deaths-nih-scientist-joe-hibbeln/
They can't both be correct, can they? Well no. Not if the comparison is apples to apples. But it isn't. What the Harvard scientists report has to do with CHD endpoints derived from epidemiological studies. In contrast, Hibbeln studies the biochemical/metabolic aspects of linoleic acid intake. It's sort of the difference between circumstantial evidence and DNA evidence in a murder trial. There are cases where the accused was convicted on the basis of corcumstantial evidence only to be exonerated years later on the basis of DNA or some other evidence that came to light.
Like Taubes and all the rest of the apologizers for saturated fats, no one can, on the basis of epidmiological studies, prove that saturated fats do not clog arteries. However, biochemistry increasingly implicates both sugar and linoleic acid. How does that work? This morning I Googled "David Brown Linoleic Acid to see what would turn up. The forth and fifth items that came up were about research some other David Brown (an actual scientist it seems) is associated with. Item 5 was especially intriguing because for a while now I have suspected that gut bacteria may mitigate the effects of high linoleic acid intake through biohydrogenation. I developed that hypothesis from studying feed research experiments involving lipids. Excerpt:
Linoleic acid (LA)
is metabolized in the human colon via conjugated linoleic acids (CLA)
to vaccenic acid (VA) (both of the latter compounds are considered to be
beneficial for health) and then to stearic acid. A similar pathway
occurs in the rumen, where this process, commonly known as
biohydrogenation, has important implications for the fatty acid
composition of meat
and milk.
http://jb.asm.org/content/189/6/2566.full
So if linoleic acid is increasingly fermented to saturated fat with increased LA intake due to remodelling of the gut bacterial profile in response to increased LA intake, this may explain why intermediate levels of LA intake appear to be harmful whereas high levels less so. It may turn out the deadliest range of intakes lies between 2% and 10% of total calories or some approximation thereof. Note, the some of the linoleic acid makes it through to the colon intact without getting absorbed into the bloodstream.
Interestingly, due to biohydrogention in the rumen, cattle do not have a high linoleic acid content in meat and fat. Poultry and swine, however, do. Feeding swine distillers dried grains plus solubles, a byproduct of ethanol production, makes their belly flap soft, so much so that feed researchers designed experiments using different sources of saturated fat in an attempt to make the bacon sliceable.
https://www.asas.org/membership-services/press-room/press-release-interpretive-summary-archive/saturated-fats-do-not-yield-better-bacon
Maybe I'm too cynical I got the impression Dr. Attia was ordering these cutting-edge-sounding tests to try to impress patients that he's using more cutting edge science than he really is like one of those modern dentistry places.
Mechanistic evidence is very weak, far from being like DNA in a trial. It's almost always possible to come up with a mechanism to support any hypothesis.This is the kind of evidence that Linus Pauling used to support megadoses of Vitamin C. What ultimately has to be studied are outcomes.
Taubes' is a very poor source if you want to learn about epidemiology. Food recall is the problem in nutritional epidemiology not the epidemology. In principle, this could be overcome for the question of LA. Virtually all body fat comes from dietary fat in humans, and humans can't synthesis PUFA. Researchers do exploit this fact to by measuring body fat to determine relative amounts of dietary fat intake in human subjects.
Check out figure 1 in this paper comparing RCTs to cohort studies: http://www.ncbi.nlm.nih.gov/pmc/articles/PMC534936/
After seeing that I'm not really with Ramsden and Hibbeln's reanalysis of one RCT, the Sydney Heart Study, when compared to numerous cohort studies.
Not sure what you mean by "mechanistic" studies. Are you referring to research that elucidates the biochemistry of inflammation? http://circres.ahajournals.org/content/107/10/1170.full If not, what sort of research are you referring to? If so, what aspect of Charles Serhan's research can be characterized as "very weak."
I find it peculiar that after nearly a hundred years of heart disease research, the world's leading scientists still do not understand what causes heart disease and how to prevent it. Perhaps it's time to pay attention to minority opinion. http://www.amazon.com/The-Modern-Nutritional-Diseases-Prevent/dp/0915241056
As macrauchenia has stated, body fat analysis has been used to assess PUFA intake because, contrary to LC lore, you are actually more like what you eat ;-) LA enrichment is seen in high PUFA diets, and you see similar with lauric acid in high coconut diets.
From the LA Veterans study: http://www.jlr.org/content/8/5/508.full.pdf
This study involved some consuming roughly 15% total energy in LA for up to 8 years. It's sort of the Grandaddy of them all, but in their attempts to blind and control -- e.g. to have the two diets be as similar in types of foods and palatability, etc. -- they used things like "filled milk" and margarine.
In contrast, laboratory experiments involving genetically similar animals raised on the same rations can paint a pretty clear picture as to what individual fatty acids do to cell function.
Basically, the disputation is about linoleic acid and saturated fat. That should be the central issue. Unfortunately, LCHF enthusiasts and vegetarians alike ignore linoleic acid research. That is why I relentlessly pursue the matter.
In the United States linoleic acid intake has risen steadily throughout the 20th century. Concurrently, there have been changes in the vitamin/mineral/fatty acid/protein content of the food supply due to fortification and the growth of the supplement industry, selective breeding of plants and animals/ variations in feed stocks used in concentrated animal feeding operations and concentrated human feeding operations (think fast food joints), refrigeration, and industrial food fabrication technology. Add to that the ever-expanding pharmaceutical industry promoting medications and pushing for mandatory immunizations and the task of sorting things out using any sort of science becomes daunting. Never-the-less, I try.
Statistically, linoleic acid intake rose steadily throughout the first half of the 20th century. Concurrently, the heart attack rate among younger males in their 30s, 40s, and 50s rose peaking around 1960 and declining thereafter. Coincident with the decline was a steep rise in linoleic acid intake and a fall in saturated fat intake.
We are about to witness a steady decline in linoleic intake thanks to research on the effects of toxic chemicals released when high linoleic acid oils are used for frying. High oleic acid versions of peanut, canola, sunflower, safflower, soybean, and corn oil are being brought to market. The transition should be complete in perhaps 10 years. If my linoleic acid hypothesis is correct, what ever else happens to the food supply, there should be a seemingly inexplicable decline in obesity and in all noncommunicable diseases. Watch for it.
I make compost. Those little critters (soil microbes) can eat a lot of material and generate considerable heat in a very short time frame. In overfeeding studies, subjects often complain about being overheated. My son-in-law, a body builder, is constantly overfeeding himself and is constantly giving off a lot of heat. In contrast, a painter once told me he tried a low-fat vegetarian diet for a while and was always cold. Conclusion: the heat released by gut microbes is actually part of the body's temperature regulating mechanism.
I used to research unabsorbed calories, a topic few seem to be interested in. Google David Brown Unabsorbed Calories and David Brown Calorie Excretion to access some of my comments.
I try to explain physiological phenomena to myself in terms of my understanding of how the real world works. Criticism of my opinions is always welcome, especially when that criticism contains a better explanation.
Regular Walking Protects The Masai -- Who Eat High Fat Diet -- From Cardiovascular Disease
There is strong evidence that the high consumption of animal fats increases the risk of developing cardiovascular disease. Many scientists have therefore been surprised that the nomadic Masai of Kenya and Tanzania are seldom afflicted by the disease, despite having a diet that is rich in animal fats and deficient in carbohydrates.
This fact, which has been known to scientists for 40 years, has raised speculations that the Masai are genetically protected from cardiovascular disease. Now, a unique study by Dr Julia Mbalilaki in association with colleagues from Norway and Tanzania, suggests that the reason is more likely to be the Masai’s active lifestyle.
Their results are based on examinations of the lifestyles, diets and cardiovascular risk factors of 985 middle-aged men and women in Tanzania, 130 of who were Masai, 371 farmers and 484 urbanites. In line with previous studies, their results show that the Masai not only have a diet richer in animal fat than that of the other subjects, but also run the lowest cardiovascular risk, which is to say that they have the lowest body weights, waist-measurements and blood pressure, combined with a healthy blood lipid profile.
What sets the Masai lifestyle apart is also a very high degree of physical activity. The Masai studied expended 2,500 kilocalories a day more than the basic requirement, compared with 1,500 kilocalories a day for the farmers and 891 kilocalories a day for the urbanites. According to the team, most Westerners would have to walk roughly 20 km a day to achieve the Masai level of energy expenditure.
The scientists believe that the Masai are protected by their high physical activity rather than by some unknown genetic factor.
“This is the first time that cardiovascular risk factors have been fully studied in the Masai,” says Dr Mbalilaki. “Bearing in mind the vast amount of walking they do, it no longer seems strange that the Masai have low waist-measurements and good blood lipid profiles, despite the levels of animal fat in their food.”
http://www.researchgate.net/profile/Per_Waendell/publication/51399410_Daily_energy_expenditure_and_cardiovascular_risk_in_Masai_rural_and_urban_Bantu_Tanzanians/links/00b7d528f4bca72c20000000.pdf
Daily energy expenditure and cardiovascular risk in Masai, rural and urban Bantu Tanzanians
Where I get stuck is that PUFA absolutely WAS more prevalent in both wild animal meats, seafood and fatty plants such as nuts and seeds. So I have a hard time with very low thresholds for LA being a culprit. Seems every time I've looked into this in greater depth, it keeps coming back to this.
Also, there's a corn oil version of the keto diet, and keto kids used to eat mayo as a food. It remains difficult again to see how this can be toxic per se.
BTW I've heard Joseph Hibbeln talk, and I was not greatly impressed. He was very anxious indeed to blame everything on linoleic acid. I suggested refined carbs and micronutrient deficiencies might play a role, and he said no, they didn't.
A scientist [well-admired on this website] advocated that just such a synthetic replacement "milk" be produced and consumed by humans—to benefit our "health",—or rather "in order to lower the blood cholesterol"—which he regarded as being equivalent:
"Why not simply get rid of the butterfat in milk and replace it with a vegetable oil rich in poly-unsaturates and low in saturates?...such milks do lower the blood cholesterol when substituted for ordinary milk in the diet..."
[the scientist was of course quite certain that:↓cholesterol →↑health]
[Ancel Keys. Eat Well and Stay Well. Rev. ed. Doubleday ©1963; p.139-140]
The side effects of keto diets seem to be independent of fat type. How about olive oil which is almost 10% LA? I am having a hard time following the logic here.
In all this, it's important not to lose sight of the basic question. Are all intakes of linoleic acid benign as the Harvard scientists assert? If so, how do we explain these observations?
"In our previous study we found that a high fat diet containing comparable amounts of soybean oil to what Americans are currently consuming caused mice to become obese, diabetic and insulin resistant and to have large lipid droplets and hepatocyte ballooning in their livers. Others had found similar results and proposed that linoleic acid (an omega 6 polyunsaturated fat) that makes up >55% of the oil was responsible for the negative metabolic effects."
"The fatty acid composition of Plenish is similar to that of olive oil (low linoleic acid and high oleic acid), which is a major component of the healthy Mediterranean diet. In the current study, we found that while a high fat diet containing Plenish also induced obesity, glucose intolerance and fatty liver, it did not induce insulin resistance as did the conventional soybean oil. It also induced somewhat less fat accumulation. Finally, we compared the diet enriched in soybean oil to an isocaloric diet that contained the same amount of total fat (40%kcal, Americans consume 34-37% fat) but with 90% of the fat from coconut oil. Those animals gained very little weight (13% versus 38% with the conventional soybean oil and 30% with the Plenish) and were not diabetic or insulin resistant. Their livers also had less fat than either of the two soybean oil diets and showed no signs of hepatocyte ballooning. Coconut oil has essentially no linoleic acid or other PUFAs." http://medicalresearch.com/weight-research/genetically-modified-soybean-oil-plenish-only-slightly-healthier/12425/
Note as far as I know, this research has not been published yet else I would have referenced the research itself.
Continuing to be clear, just because Keys was a tireless researcher, smart as hell,
and a formidable opponent in the dietary wars (IMO) doesn't mean I also consider
him to have been admirable. Your guess [above] was wrong; Keys wrote: "The non-fat part of milk is an unsurpassed food for old and young alike;"...the only thing wrong with milk [in Keys' view] was its fat—that fraction that contained the indispensable vitamins A, D, E, and K₂, and why? because "butterfat
is almost unequalled as a dietary promoter of cholesterol in the blood." [p. 136 from Eat Well and Stay Well.]
Keys seems to have been the real beginning of the never-ending diet-wars, that battle
of Fat vs Carbs as to which will be shown to be our true Dietary Public Enemy No.1—that battle which—as you know!—continues on down to the present. Opinion divides. Fiercely. And often reminds me of another opposition—the two opposite ways the world could end—that Frost wrote about in his poem "Fire and Ice":
Fat and Carbs [with apologies to Robert Frost]
Some say our health is wrecked by fat,
Some say carbs,
Ancel Keys assured us that
We'd kill ourselves with dairy fat.
But critics thought such claims were lies:
"Fat", they said, "was good! Instead—
It's carbs that hasten our demise."
(You're doubly dead from buttered bread).
"The most consistent and significant lipid change observed in the brain of copper-deficient rats is a higher proportion of linoleic acid in the phospholipids, particularly PC, of isolated myelin and tissue from all brain regions. Of equal significance is the lower level of 22:6(n-3) in the PC and PE of the cerebellum."
http://jn.nutrition.org/content/122/1/65.full.pdf
In other words, what looks like linoleic acid toxicity could actually be copper deficiency. Which most Americans appear to have.
"The Western diet is often low in copper,3 according to the pooled data from several articles on more than 900 diets chemically analysed. About 62 and 36% of diets of 80 randomly selected adults in Baltimore4 were below the recommended dietary allowance and the estimated average requirement for adults, respectively, 0.9 and 0.7 mg daily."
http://eurheartj.oxfordjournals.org/content/27/1/117.1
You said no doubt a number of deficiencies can cause heart disease. Perhaps, but none as convincingly as copper deficiency. More than 80 similarities have been found between humans with ischemic heart disease and animals with copper deficiency. Your Dr Williams should know this.
So deficiency may come from more than dietary inadequacy.
You can't expect Dr. Williams to be aware of research (1992) published after his death (1988). Do you know of any copper deficiency research that Williams might have had access to prior to the 1973 publication of the book I quoted from.
Here's a brief history of copper research in relation to heart disease.
http://jn.nutrition.org/content/130/2/489S.full
A quote that might interest you:
"A short time later, Ball et al. (1963) began to publish changes in cardiovascular anatomy found in mice fed a diet high in lard in Mississippi. Atrial thrombosis was most obvious, but coronary necrosis, coronary thrombosis, myocardial necrosis and ventricular calcification also were found. Mortality was high. Two decades later, it was found that adequate dietary copper (Klevay 1985) could prevent the atrial lesions and eliminate premature mortality. Copper was an antidote to fat intoxication."
I rather think Ball's experiments were what clinched the diet-heart idea. If mice fed lard got heart disease, saturated fat was the culprit. Why nobody listened to Klevay when he showed it was copper deficiency, I don't know.
I'll study this and we'll see what questions it raises.
Copper deficiency can cause iron overload, and iron overload has been found in many common diseases. Obesity, diabetes, heart disease, Alzheimer's, arthritis ... the list goes on.
This 1983 study at the M.I.T. Clinical Research Center [published in Metabolism] comes pretty close:
S.D. Phinney, G.L. Blackburn, et al. The Human Metabolic Response to Chronic Ketosis Without Caloric Restriction: Physical and Biochemical Adaptation.
http://www.sciencedirect.com/science/article/pii/0026049583901051
Nine lean healthy men were fed a eucaloric ketogenic diet [EKD] for four weeks:(1.75g/kg protein per day, with carbs restricted to <20g/day; calories given at 35-50 calories/kg/ day; thus, 83% to 85% of the total calories came from fat):
"The daily diet was composed of three meals and a snack. The subjects were given their choice from five meals prepared from ground beef, breast of chicken, water-packed tuna, powdered egg solids and cheddar cheese. Mayonnaise, heavy cream, sour cream, and cream cheese were used as the primary lipid sources.
[The mayo was probably Hellman's, and so its soybean oil would have unfortunately provided some linoleic acid, but most of the fat in this ≥83% fat diet was indeed high saturated dairy fat.]
As to your question re the side effectsof such a pretty hefty sat-fat ketogenic diet, in the Discussion we read:
"In view of the tests done to screen for ill effects of the EKD, the remarkably benign nature of a diet providing 85% of calories as fat is notable. After four weeks there was no measurable impairment of hepatic, renal, cardiac, or hematopoietic function. The serum uric acid level, elevated by competition from ketone bodies for excretion, was almost back to normal by that time. The rise in the serum cholesterol level [from 159 to 208mg/dl] however, appeared sustained, while triglycerides fell from 107 to 79mg/dl...Depending on the specific meal choices selected, the daily cholesterol intake may have approached 2g for some subjects. Nitrogen balance was regained after brief adaptation, serum lipids were not pathologically elevated, and blood glucose oxidation at rest was measurably reduced while the subjects remained euglycemic."
Relevance?
Meanwhile, mongongo nuts that are a reported dietary staple were brushed off. I'll try and return to this discussion at some point.
I meant that it would seem odd to me for Keys to advocate for a fake food rather than leave a food out altogether, but it's a semantics game at this point.
Dairy has always been a rather interesting food to me. It has a mixed nutritional resume, though mostly positive associations. Still it is a food that when I think about it makes little sense for adults. I mean it is infant food for a wide range species with extremely varied adult diets/nutritional requirements. There's little doubt it wouldn't have been part of our genetic adaptation until somewhere in the 6-9k year ago mark, and there are cultures who don't include any dairy in them yet are healthy and long lived.
Keys did research starvation and nutrition from that perspective in his earlier works.
"Swapping saturated fat and carbohydrates for linoleic acid – the main polyunsaturated fat found in vegetable oil, nuts, and seeds – lowers risk of coronary heart disease, according to a new study by Harvard School of Public Health researchers." http://www.hsph.harvard.edu/nutritionsource/2014/11/05/dietary-linoleic-acid-and-risk-of-coronary-heart-disease/
And the article about polyunsaturated fat says "Most people don’t eat enough healthful unsaturated fats. The American
Heart Association suggests that 8-10 percent of daily calories should
come from polyunsaturated fats, and there is evidence that eating more
polyunsaturated fat—up to 15 percent of daily calories—in place of
saturated fat can lower heart disease risk." http://www.hsph.harvard.edu/nutritionsource/2014/11/05/dietary-linoleic-acid-and-risk-of-coronary-heart-disease/
The entire article contains no mention of omega-6 or linoleic acid. Do you still maintain it is disingenuous to bring CO into the picture?
There are many outlandish claims made about the healthfulness of coconut oil as well, but my point is that it IS disingenuous to look at CO as a representative saturated fat. Further it's disingenuous to use the Tokelau and Kitivans as examples most times too, as they ate coconut, didn't slurp spoonfuls of oil.
From the Facebook conversation:
http://circ.ahajournals.org/content/early/2014/08/14/CIRCULATIONAHA.114.011590
Diets high in animal protein do increase the chance of forming both uric acid and calcium oxalate (which make up the vast majority of kidney stones). But as you know, a proper ketogenic diet will not be high in protein [an anti-ketogenic factor]—rather, a diet high in fat.
Even so, consider the Rock Candy Principle: If you ordinarily try to combine 2 cups of sugar into 1 cup of water, it won't all go into solution. But if you heat the water, you can put more sugar into it than it would normally absorb, i.e., you have made a
supersaturated solution—there is now more sugar in the water than can stay in solution for any period of time. If you now place a string inside the pot, that string will act as the promoting factor that starts the sugar crystals forming, = "rock candy." The same thing applies to the formation of calcium oxalate kidney stones.
The common assumption that water in equals water out applies if and only you a. are not active, b. don't get hot, c. aren't out on the beach or desert, d. aren't perspiring heavily, etc. In such cases water in will certainly not equal water out. When you sweat, your kidneys reduce urinary volume, making your urine more concentrated—heading you towards that potential of an unwelcome urinary supersaturated solution.
Having a dilute urine is overwhelmingly important because no one will get a kidney stone if his or her urine is sufficiently dilute, regardless of his or her intake of purine-containing animal protein or high-oxalate foods. Kidney stones are thus no more a genuine side effect secondary to ketogenic diets than of jogging on the beach or doing outdoor work in Arizona. A good rule of thumb is to drink enough water to produce a urinary volume of 2 liters/day. The National Kidney Foundation advises even more—a daily pee volume of 2.5 liters per day.
This
discussion thread began about 5 days ago with a comment about replacing
SFA with PUFA. I noted that the Harvard group characterizes all SFAs as
unhealthy. There was discussion about what happens to n-6 fatty acids in
the digestive tract. I brought biohydrogenaton into he picture, then
unabsorbed calories. You brought up the keto kids matter. I noted there
were side effects associated with the PUFA-rich fats used to treat
convulsions. I then suggested it might be useful to replace
polyunsaturated fats with CO because you said side effects seemed to be
independent of fat type. I referenced the UCR murine research to make a
point that CO seems to be more benign than n-6 PUFA. Then, you said, "CO has such a different fatty acid profile from most sources of
saturated fat, I think it is disingenuous to even present it as such
without noting that, while saturated, it is actually rather low in the
LCSFA's compared to animal sat fat sources." Then you said, "...it IS disingenuous to look at CO as a representative saturated fat."
I never implied that we "look at CO as a representative saturated fat." If you're not certain you grasp my meaning, ask for clarification rather than attach an interpretation based on conjecture.
E.V. McCollum—describing in his own words how he discovered vitamin A:
http://www.annualreviews.org/doi/pdf/10.1146/annurev.bi.22.070153.000245
By reason of a combination of defects in my technic my rats were able to distinguish clearly between the value to them of butter fat and egg-yolk fat, in contrast to olive oil and lard. They fared markedly better nutritionally on the two former than on the two latter adjuvants to the diets. This study Miss Davis and I published in 1913. It afforded the first evidence that certain fats contain an indispensable nutrient hitherto unsuspected. Some months later Osborne & Mendel described experiments which confirmed our discovery that certain fats contain an unidentified nutrient essential for the nutrition of the rat. Of special interest was our transfer of this nutrient from butter fat to olive oil. Butter fat was saponified in alcoholic KOH and the resulting soap was dissolved in water and olive oil was thoroughly emulsified in the soap solution. The olive oil was of the same sample as had been tested on rats and found of no value to them. The emulsion was then broken with ether, and the olive oil was recovered in that solvent. After removing the ether the olive oil was found by feeding tests to have acquired the nutritive quality of the butter fat...this nutrient, now known as vitamin A...
Evelyn wrote: "Still it [milk] is a food that when I think about it makes little sense for adults. I mean it is infant food for a wide range species with extremely varied adult diets/nutritional requirements."
McCollum addressed this in Chapter XVI, in his the Newer Knowledge of Nutrition:
"Any diet which is unsuited for the promotion of growth in the young will not be satisfactory for the maintenance of health in the adult...Any diets which we have studied, which were not satisfactory for the promotion of growth in a young rat, were found to cause some damage to adults which were restricted to them. This might be manifested in early aging, short life, lowered fertility, or the deterioration of a family restricted to it for several generations...a diet may be sufficiently good to enable an animal to grow in a perfectly normal manner, and to exhibit a moderate amount of fertility, yet with each succeeding generation the progeny becomes smaller and less well developed physically, and after two, three, or four generations the strain dies out.
...The most surprising generalization which is warranted by exact nutrition studies, is that even a diet composed of cereal grains, legume seeds, tubers, fleshy roots, fruits and muscle cuts of meat, irrespective of the proportions in which the components are represented, the variety it affords, or the chemical composition...will fail to support satisfactory growth in a young rat...Such a diet may contain any or all of a list of foods including wheat, maize, rolled oats, barley, rye, pea, bean, soy bean, potato, turnip, radish, beet, steak, ham, roast,etc., or any other seed, tuber root and muscle meat, and still fail signally to maintain the vitality of a rat." And just what then are the deficiencies of such a diet? "...calcium, sodium, chlorin, and fat-soluble A."
McCollum found that the addition of milk unfailingly corrected the deficiencies in such diets. Diets which are of course typical of many adults today.
Which is why he frequently wrote: "There is no substitution for milk."
Diets high in animal protein do increase the chance of forming both uric acid and calcium oxalate (which make up the vast majority of kidney stones). But as you know, a proper ketogenic diet will not be high in protein [an anti-ketogenic factor]—rather, a diet high in fat.
Even so, consider the Rock Candy Principle: If you ordinarily try to combine 2 cups of sugar into 1 cup of water, it won't all go into solution. But if you heat the water, you can put more sugar into it than it would normally absorb, i.e., you have made a
supersaturated solution—there is now more sugar in the water than can stay in solution for any period of time. If you now place a string inside the pot, that string will act as the promoting factor that starts the sugar crystals forming, = "rock candy." [You definitely know your chemistry, and this will be completely familiar to you]. The same thing applies to the formation of calcium oxalate kidney stones.
The common assumption that water in equals water out applies if and only you a. are not active, b. don't get hot, c. aren't out on the beach or desert, d. aren't perspiring heavily, etc. In such cases water in will certainly not equal water out. When you sweat, your kidneys reduce urinary volume, making your urine more concentrated—heading you towards that potential of an unwelcome urinary supersaturated solution.
Having a dilute urine is overwhelmingly important because no one will get a kidney stone if his or her urine is sufficiently dilute, regardless of his or her intake of purine-containing animal protein or high-oxalate foods. Kidney stones are thus no more a genuine side effect secondary to ketogenic diets than of jogging on the beach or doing outdoor work in Arizona. A good rule of thumb is to drink enough water to produce a urinary volume of 2 liters/day. The National Kidney Foundation advises even more—a daily pee volume of 2.5 liters per day.
My comment was specific to O6s being cited as culprits in neurological disorders, and yet O6 oils have been used to treat them. The implication was therefore that perhaps they were responsible for side effects. This is a distraction, as even if they caused all the other bad things, they still benefit the neurological condition.
Ketogenic Diets: Treatments for Epilepsy and Other Disorders
This book is a good reference for those considering keto for neurological disorders. Discusses a modified Atkins (35% protein) approach as well.
Mainly, I try to stand up for what's right. To be able to do so, a person needs to be dedicated to figuring out how the real world works. The only reason I'm lurking on this site is because you, Jane and a few others have a different perspective on things. You know things I don't and have thought thoughts I haven't.
I'm currently studying the circulation article you linked to. http://circ.ahajournals.org/content/early/2014/08/14/CIRCULATIONAHA.114.011590 I must have read commentary on that article rather than the article itself, perhaps just the abstract.
From the article:
"The association between dietary circulating LA concentration was nonlinear (P<0.001). Circulating LA showed the greatest dose-response association with intake of LA up to ~8% of total daily energy; with relatively smaller increases at intakes>8%."
This sort of observation suggests biohydrogenation or fatty acid excretion or both may come onto play at higher intakes of LA. What we need to know is whether higher intakes of LA are associated with overall higher overall fat intake and lower carbohydrate intake. If that's the case, the gut microbe profile would remodel accordingly making biohydrogenation a distinct possibility.
Would you be interested in doing a post on Linoleic Acid research (or perhaps fatty acid toxicity), exploring the evidence for and against the Harvard group's recommendation to swap linoleic acid for saturated fat? Jane's material on mineral depletion might also shed light on the problem of fatty acid toxicity in general and linoleic acid toxicity in particular.
Thanks
Keto enthusiasts who think that omega-6 is a culprit will reply that it's the general replacement of mostly glucose oxidation by FFA's—and, of course, ketones—that is responsible for the main benefits for the various neurological conditions, i.e., the replacement of glucose (resulting from a very low carb intake) is the chief factor that delivers the neurological benefits,—even when the person chooses a dangerous fat like linoleic acid—but that it would be better still to have relied on the more stable saturated fats for one's majority lipid supply. Early literature from doctors employing ketogenic diets for epileptic children instructed their parents to immediately regard heavy whipping cream as its own food group, since it was an easy and more palatable way to get a lot of fat into their child's diet. (You can't whip corn oil, or make a sugar-free soybean oil frozen dessert, or a safflower oil "milkshake".)
"Ketogenic Diets: Treatments for Epilepsy and Other Disorders
This book is a good reference for those considering keto for neurological disorders. Discusses a modified Atkins (35% protein) approach as well."
Yeah, I've had several editions of Dr Freeman's book, the 5th edition of which does indeed discuss the use of a "modified Atkins diet" [actually, the protein for this is
30%—not 35%—see the comparison pie charts on p. 201—but even a 30% level is way more protein than their previous standard ultra-extreme anti-seizure ketogenic diet—i.e., 8% protein/90% fat]. As to whether a parent should follow the prevailing consensus to avoid saturated fat, Freeman does give a brief nod to this idea—but
then immediately discounts its importance:
"We recommend that you use as many unsaturated fats as possible, such as canola, safflower, flaxseed, or olive oil, or margarine made from canola oil. However, no research exists on the effect of a diet comprised of 90% fat, whether saturated or unsaturated. No data indicate that the ketogenic diet, despite its high fat content, leads to heart disease or atherosclerosis later in life." [p. 254]
With regard to high cholesterol and other lipid abnormalities: "...in about 30% of children there may be cholesterol and triglyceride levels that exceed current recommendations for normal children, but in most cases this is a transient finding...[and after period of adjustment]..."the levels begin to stabilize and then return very close to pre-diet levels...We have had virtually no child discontinue the diet exclusively for lipid abnormalities, and have never yet treated a child on the diet who has markedly elevated cholesterol with statin medication." [p. 167]
In terms of dose-response curves, there are any number of variables that can explain a non-linear relationship. Many "biomarkers" display similar behavior.
When I began writing essays about nutritional controversies several decades ago, I asked our pastor to evaluate my work. The first thing he said was, "Never insult your audience." So I try not to do that, ever. I will, on occasion, make the point that in matters controversial, relying on consensus of opinion can be problematic as compared to taking time to investigate the matter thoroughly.
The linoleic acid controversy exists. The alternatives are to choose up sides or read the literature. And by read the literature, I mean read all points of view. John Stuart Mill put it this way.
In the case of
any person whose judgement is really deserving of confidence, how has it
become so? Because he has kept his mind open to criticism of his
opinions and conduct. Because it has been his practice to listen to all
that can be said against him, to profit by as much of it as was just,
and to expound to himself and upon occasion to others, the fallacy of
what was fallacious. Because he has felt that the only way in which a
human being can make some approach to knowing the whole of a subject is
by hearing what can be said about it by persons of every variety of
opinion and by studying all modes in which in can be looked at by every
character of mind. No wise man ever acquired his wisdom in any mode but
this; nor is it in the nature of the human intellect to become wise in
any other manner.
I have no idea what you meant by "Evelyn's science is far better than you (I) think it is." I do think that both you and Evelyn are far smarter than I and you folks know things I don't. That is why I appreciate the interaction.
In my quest for an understanding of how the real world works I have read a great deal over the past 38 years. I have ranged far and wide trying to understand why our best scientific minds have not been able to figure out what causes noncommunicable diseases. The answers are there. Of that much I am certain.
I recommend "The Modern Nutritional Diseases: And How to Prevent Them. By Fred and Alice Ottoboni." These two retired public health scientists are masters of explanation. I don't, however, agree with everything they say. I do not favor the ketogenic approach. It seems to be therapeutic over the short haul just as the low-fat vegan approach can be therapeutic. But day to day eating needs to emphasize whole foods with high (Brix) mineral content.
http://www.ncbi.nlm.nih.gov/pmc/articles/PMC3604685/
http://www.ncbi.nlm.nih.gov/pmc/articles/PMC3206402/
http://www.ncbi.nlm.nih.gov/pubmed/18710653
Meanwhile, is this you or the other David Brown?
http://www.bmj.com/rapid-response/2011/10/31/unabsorbed-calories-important-consideration
I don't know what you are lobbying for here. You have no clue what degree I've looked into this topic, and I'm sorry that I can't give you whatever recognition you seem to be seeking. I have other priorities.
You have erroneously jumped to the conclusion that I have chosen up a side and that this choice is made out of ignorance. Please list in one post all of the literature you deem necessary for one to consider before they will be considered "thorough".
Other David Brown? Apparently, although there are many David Brown's in the world, I'm the only one who writes about the unabsorbed calories (not particularly interested in that any more), the saturated fat controversy, and linoleic acid research. Were I interested in drawing attention to myself, I would have written a book. As it is, I didn't want to write the article for Ecologist magazine. I requested the editor write an article about the omega-6 controversy. We've corresponded for about 10 years and I've sent quite a bit of information about omega-6 his way. He put it back on me so a year later I wrote the only article I have ever written for an actual magazine. I don't count opinion pieces as articles.
I write several hundred messages a year to scientists and journalists who bash saturated fats or extol linoleic acid. It takes up a lot of my time. I kind of enjoy doing it but would quit in a heartbeat if the saturated fat/linoleic acid problem were resolved.
I love extreme gardening and inventing ways to make gardening more efficient and the food more nutritious. Pictures of my front yard published on this site. http://theconsciouslife.com/omega-6-friend-or-foe.htm
I'm trying to make sense of your request to "list in one post all the literature I deem necessary for one to be considered thorough." To me, being thorough is an ongoing process. I would never call someone ignorant who has not delved as far into the subject matter as I have. That is insulting. I do not insult. But I do challenge others to produce evidence that supports opinions. which you have done on occasion. Thank you. But in addition to the evidence itself, I desire a reasoned argument regarding the validity of that evidence. Perhaps more importantly, I look for a reasoned argument against my own evidence and arguments.
What I dislike is the weight-of-the-evidence argument, as though validity can somehow be measured by the number of scientific papers published on the subject.
I will be happy to furnish scientific papers on linoleic acid research. However, I would prefer to do it in two posts. First, the pro linoleic acid research material. I would request you add to it any pro LA research you are familiar with. Next, I would list the evidence against LA and request you list any research I may have missed. That way, we both end up less ignorant.
The answer is really quite obvious: they thought it was due to genes and could be fixed with gene therapy. This is what the Human Genome Project was all about.
saturated fats and ignore the actual cause of heart disease (mostly
excessive consumption of added sugars and omega-6 seed oils) I will
labor to influence public health policy and familiarize Americans with
the truth about fats and sugars."
Are you planning to rewrite this to include something about copper deficiency?
Is the Human Genome Project the "better science" you referred to? And if so, how does that relate to the saturated fat controversy and the omega-6 issue. The newer (Genome) science has little to do with efforts to stem the tide of noncommunicable disease currently sweeping the world. This does. "Swapping saturated fat and carbohydrates for linoleic acid – the main polyunsaturated fat found in vegetable oil, nuts, and seeds – lowers risk of coronary heart disease, according to a new study by Harvard School of Public Health researchers." http://www.hsph.harvard.edu/nutritionsource/2014/11/05/dietary-linoleic-acid-and-risk-of-coronary-heart-disease/
I could be wrong but it seems to me the Human Genome Project is all about correlating biochemical and physiological make up with individual responses to various configurations of nutrient intake so as to be able to prescribe an appropriate dietary regimen from birth onward. It's the "One man's meat is another man's poison" principle as discussed in "Biochemical Individuality" by Roger J. Williams, PhD and in "Nutrition and your Mind" by George Watson, PhD. Have you read these books?
I haven't posted anything on my blog since 2011. I've left it up as a record of my educational efforts up to that point. Guess it's time for an update with the copper deficiency problem given a place of prominence.
I just Googled "Copper Deficiency and Heart Disease" and brought up some interesting looking articles. Is there anything else I could Google that would connect me with good quality research on copper deficiency diseases?
Are you thinking linoleic acid may be problematic or do you agree with Frank Sacks? "Omega-6 fatty acids lower LDL cholesterol (the “bad” cholesterol) and reduce inflammation, and they are protective against heart disease. So both omega-6 and omega-3 fatty acids are healthy. While there is a theory that omega-3 fatty acids are better for our health than omega-6 fatty acids, this is not supported by the latest evidence. Thus the omega-3 to omega-6 ratio is basically the “good divided by the good,” so it is of no value in evaluating diet quality or predicting disease." http://www.hsph.harvard.edu/nutritionsource/omega-3/
In looking at the latest evidence it looks like the risk for heart attack rises and than falls as plasma linoleic acid goes from 15% to 25% of plasma phospholipids. (Figure 2) http://circ.ahajournals.org/content/early/2014/08/14/CIRCULATIONAHA.114.011590.full.pdf+html
It's important to note that there is no data for values lower than 15% because there are no randomized controlled trials comparing the effects of low (pre-industrial - 2%) and high (currently 7.5%) intakes of LA. http://www.karger.com/Article/FullText/324749
The Human Genome Project was sold to politicians (eg Tony Blair) as part of the biotechnology revolution which would 'cure half our diseases and prevent the other half' (Blair quote). We would get rich selling our cures abroad. It was crap, and lots of scientists knew it.
I don't see a deliberate attempt to make people unhealthy so as to make money for the medical industry, if that's what you implied. In other words, given a choice between explaining what has taken place in terms of either ignorance or wickedness, I would choose ignorance because it is so prevalent. Thomas Jefferson said, "Enlighten the people generally, and tyranny and oppressions of body and mind will vanish like evil spirits at the dawn of day."
Assuming I'm correct. The consequences of not adequately assessing the effects of industrial tampering with the food supply are no less pernicious in terms of their consequences for human health.
It is argued that the Dietary Guidelines for Americans have little impact on the health of Americans because very few people pay attention to them. But government policy is based on those guidelines. From this morning's news: "By law, schools are required to provide specific amounts of protein, calories, whole grains, fruits and vegetables, based on a student's grade level, and also provide fat free or low-fat milk. Meals are also required to have reduced amounts of sodium, saturated fat and trans fat."
My chief aim is to correct the Dietary Guidelines for Americans as soon as possible because they affect how food is configured in schools, prisons, and hospitals throughout the country, indeed, throughout the World. In addition, the fat content of the the food supply is configured according to those Guidelines. Ironically, the edible oils industry is making their products more benign in terms of linoleic acid content even as Harvard researchers tout the benefits of swapping linoleic acid for saturated fats and carbohydrates.
Assuming you disagree, what alternative course of action do you propose? If you agree, how can we work together to move things in the right direction?
Your health improved when you cut down on linoleic acid, and you think that makes you a better judge than McCarrison of what people should eat.
I am not in the least surprised you want to work with me. I would be very useful indeed, with my scientific background. No chance, pal.
I have three (or is it 4) books about the Hunzas. Their diet contained modest meat intake. But all their food was mineral rich due to the mineral profile of the soil, their practice of composting everything and the (supposedly) mineral-rich "glacial milk" they drank and irrigated their crops with. Fred Miller and McCarrison before him pretty much had it nailed down in terms of what is required for optimum health. From "Healthy Teeth Through Proper Nutrition": "...Sir Robert showed that the Sikhs and Pathans, who lived amidst filth and poverty, still grew into a healthy, strong, robust race. Their diet consisted mostly of sour milk curds, chappaties (whole wheat cereal), leafy vegetables, some meat, citrus fruits, and yellow vegetables and fruits."
When McCarrison was conducting his research, soybean oil was not ubiquitous in the food supply. However, when J.I. Rodale wrote about the Hunzas, soybean oil consumption was rising steeply. You know what happened to him, don't you? He died from a heart attack during taping of a segment of the Dick Cavett Show. http://opinionator.blogs.nytimes.com/2007/05/03/when-that-guy-died-on-my-show/?_r=0
My second favorite biochemist, (You haven't read his books?) Ross Hume Hall, was a vegetarian. He died from prostate cancer at age 76. In our initial correspondence we discussed McCarrison. And he was well aware of the omega-6 problem. However, vitamin D research had not advanced very far when he was first diagnosed with cancer. https://csmb-scbm.ca/bulletin/pdf/Bulletin03/Obituary42-46.pdf
Paul Stitt was likely another victim of excessive polyunsaturated fat intake. He was my age when he died from cancer. He was somewhat anti-saturated fat and pro flax seed. http://professing.proboards.com/thread/13119/paul-stitt
Do I have this right? You don't think linoleic acid is problematic? You believe refined carbs (which we agree upon and the government is finally concerned about) and meat are responsible for most of our ills? Do you think the saturated fat in dairy is harmful? I know where you stand on mineral content of food. We're on the same page there. What I'm after is documentation for your position on meat seed oils intake.
In closing, David Ramsey brought this to my attention. This is so well said. https://www.t-nation.com/diet-fat-loss/fat-that-makes-you-fat
Ramsey used (misrepresented) my comments on linoleic acid to criticize the article. I am not an authority. Opinion never constitutes authority. Only the facts matter. Aragon did an excellent job of setting the record straight on linoleic acid. I agree with virtually everything he said in the article and that, my friend, is saying a lot.
Anyway, from my peripheral position to the discussion, the problem with pointing the finger of doom at O6 or linoleic acid is that it's confounded by the issue of partial hydrogenation and transfats. Is it the seed oil consumption, or the transfats?
And note: commercial peanut butter (at least until recently) contained partially hydrogenated oils.
http://www.ncbi.nlm.nih.gov/pubmed/9681949
Saturated fat increases iron absorption and inhibits manganese absorption. Have a look at this paper. The saturated fat (stearic acid) was compared to high-linoleic safflower oil, which does the opposite. This is one of the reasons I have doubts about the toxicity of linoleic acid.
http://www.ncbi.nlm.nih.gov/pubmed/11697763
You might also like to look at this interview of Ron Krauss on saturated fat and red meat. He has found that either alone is OK but the combination is very much not OK. He thinks it's the effect of saturated fat on iron absorption that's the problem.
http://www.meandmydiabetes.com/2012/04/17/ron-krauss-saturated-fat-red-meat-it-depends/
I was familiar with the Ron Krauss interview. However, reading it again with an awareness of the iron/manganese balance issue furnishes a different perspective on things.
I study animal feed research because feed researchers seem to have a better grasp if lipid and mineral deficiency/balance issues than human nutrition researchers. It may be that some of the principles learned can be transferred to human nutrition. For example, today I found this comment in Chapter 14 (Manganese) of a book entitled Mineral Nutrition of Livestock by N.F. Suttle. "High dietary iron is probably a risk factor for manganese deprivation in all species."
Again, thanks for helping me become a little less ignorant.
http://www.ncbi.nlm.nih.gov/pubmed/23372018
The research on Alzheimer's is if anything even more interesting. There is a key enzyme called PP2A (protein phosphatase 2A) which was known to play a major role in Alzheimer's. It's a manganese enzyme. It has now been found to be necessary for clearance of aggregated proteins (by autophagy) in neurons.
"These data are important to human neurodegenerative diseases, especially Alzheimer's disease, because they provide links for the first time between the pathological features of Alzheimer's disease: PP2A downregulation, autophagy disruption, and protein aggregation."
http://www.ncbi.nlm.nih.gov/pubmed/22892312
This is what I wrote on the longecity forum just yesterday, as a summary of sorts:
"Believe me, it is not the first time I run across those studies. I
have been there years ago, when the omega-3-hype first made its waves,
seen it all, read all the literature, felt exited for a short peroid of
time - but then I took a step back and looked at the larger picture
again, considering the epidemiology and clinical trials and found them
to hardly support the grandiose thesis put forth by some authors.
There is a large body of epidemiological evidence
showing that substituting saturated fats or even refined carbohydrates
with PUFAs reduces mortality risk and/or several specific disease risks.
Most epidemiological studies do not adequately differentiate between
omega-6 and omega-3, but the positive effects tend to be more pronounced
in countries with a high traditional consumption of omega-3-rich plant
oils and fish (e.g. Japan and Mediterranean countries). Ramsden's et al. meta-analysis of PUFA intervention trials
- particularly their dissection of the Sidney Diet Heart trial in
contrast to the singularly sucessful Lyon Diet Heart Study - has nicely
complemented the epidemiological evidence, showing that the subtitution
of saturated fat with a balanced amount (1:5 alpha-linolenic to linoleic
as found in soy and walnut oil seems to suffice) of PUFAs significantly reduced the
risk of CVD and all-cause mortality, while only the imbalanced ones,
providing almost exclusively linoleic acid, tended to fail.
The fact, though, that the omega-6-trials didn't fail more badly,
tells us that even an excessive intake of linoic acid from refined plant
oils can't be much worse than the usual excessive intake
of saturated fats or refined carbohydrates. All things considered, the
lesson learned should be not to obsess about macronutrients and abstract
ratios, but to eat a whole food, predominantly plant based diet,
including at least one good plant source of omega-3 (e.g. flaxseed),
complemented by a small amount of HUFAs from fish or algae oil."
Post a Comment
Comment Moderation is ON ... I will NOT be routinely reviewing or publishing comments at this time..